
You don’t need an expert to tell you obesity has become a major health problem worldwide. The World Health Organisation estimates 35% of the world’s adults are overweight and 11% obese, double the rate in 1980.
Overweight and obese people have an increased risk of high blood pressure, type 2 diabetes and cardiovascular disease, as well as arthritis, obstructive sleep apnoea and liver disease. Obesity can reduce life expectancy by five to 20 years, and the obesity epidemic may soon reverse the gains that have been made in human longevity.
We could simply eat less and move more. But, of course, it’s not that simple; many of us find it impossible to consistently control our calorie intake. For those with severe obesity or diabetes who have tried all other medical options but failed to lose weight, bariatric surgery is the last-line option.
Bariatric surgery refers to a group of surgical procedures that make it more difficult to over eat and/or absorb food. It is recognised as the most effective treatment for obesity, resulting in both the largest and most sustained weight loss, and the greatest reduction in obesity-related disease and death.
But it is highly invasive, it comes with a number of risks and in some cases is not effective.
Types of surgery
There are three main types of bariatric surgery available in Australia: laparoscopic adjustable gastric band (LAGB), sleeve gastrectomy and gastric bypass. All of these procedures can now be performed with keyhole surgery.
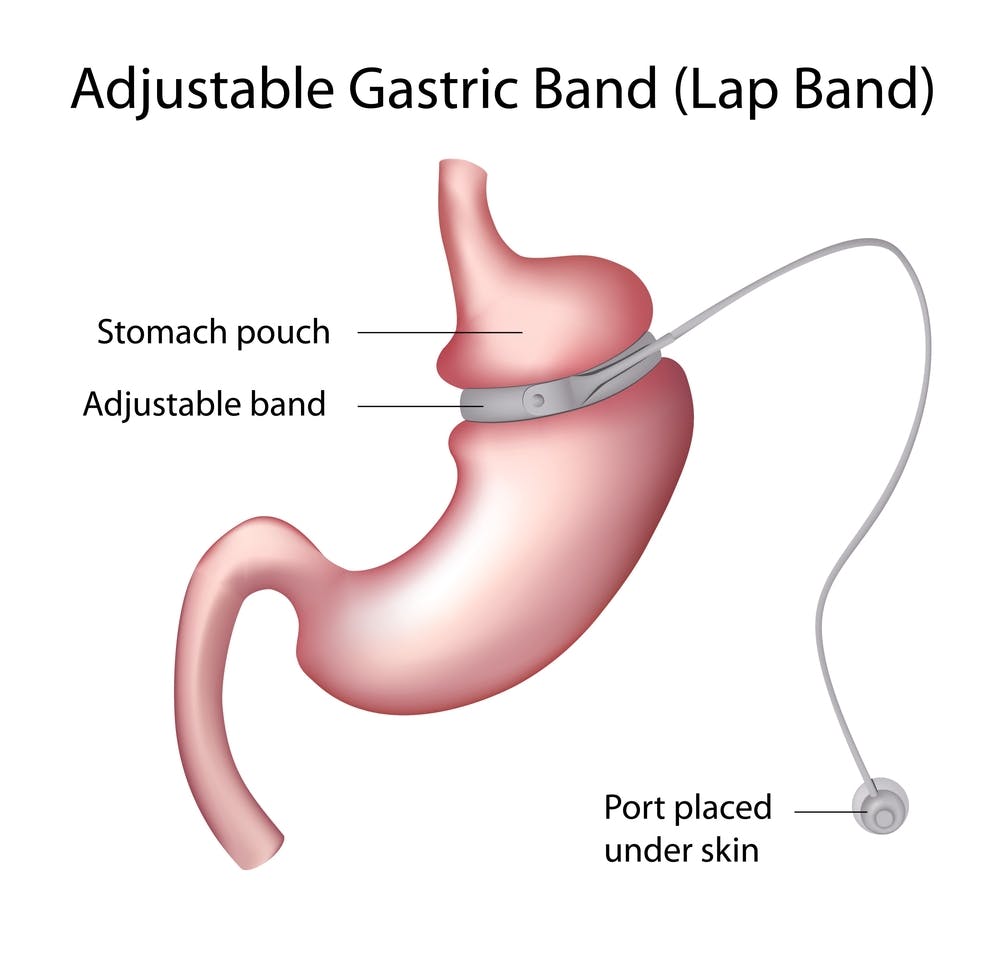
Laparoscopic adjustable gastric band
LAGB is a relatively simple operation in which an adjustable silicone balloon ring is placed around the upper stomach. As well as restricting the volume of food the stomach can hold, the pressure created by food in the reduced upper stomach stimulates the vagal nerve, reducing appetite.
But it is easier to consume fluids than denser, healthier foods, reducing the quality of the diet, which might explain why LAGB results in less weight loss than other procedures.
For sustained weight loss, close follow up is needed, with optimal adjustment of the band; if the band is too tight, it’s difficult to eat healthy foods and obstruction may occur, if the band is too loose, appetite is not controlled.
Revision surgery is required in about 15% of patients within three years due to band slippage and erosion of the band into the stomach wall.
Side effects include gastric reflux.
Sleeve gastrectomy
In this procedure, most of the stomach is removed. It is technically simple and is reported to have a good safety profile in experienced hands.
The weight loss and improvement in diabetes is related to both reduced capacity of the stomach and an increase in hormones that reduce appetite and increase meal related insulin release.
Nutritional deficiencies are common and most people need supplements of nutrients normally absorbed by the stomach. Surgical complications include leakage or bleeding at the suture line.
This procedure is the newest and there is less long-term data than for other procedures.
Gastric bypass
This operation creates a small proximal stomach joined to the end of the jejunum (the lower small bowel) so that parts of the small bowel, where nutrients are absorbed, are bypassed. While a more extensive operation, it can be reversed because nothing is removed.

Gastric bypass results in more weight loss than the sleeve gastrectomy as there is both a reduction in the capacity of the stomach and reduced absorption of nutrients, including the beneficial changes in gut hormones seen with the sleeve gastrectomy.
In some patients, the weight loss is so great that they become malnourished and all patients require life-long supplements of vitamins, calcium and other minerals. There is also the risk of “dumping syndrome” due to the rapid transit of undigested food from the new, smaller stomach to the bowel, causing nausea, cramps, diarrhoea, and occasionally low blood sugar from very high insulin levels.
Surgical complications include leakage, bleeding and bowel obstruction.
Risks and long-term effects
In addition to the complications of surgery and malnutition, the long-term effects can include reduced bone density and impairment in nerve function.
There is also a reported increased incidence of suicide and substance abuse in patients who have had bariatric surgery. But there have been few controlled studies comparing the quality of life after surgery with patients who have not sought surgery.
It’s important to note that individuals do not need to attain the amount of weight loss achieved with surgery to have substantial beneficial health outcomes. A reduction in weight of 5% to 10% can improve the health of your heart and reduce obesity-related disease and early death, especially if combined with increased physical activity.
Eligibility
The current guidelines in most countries, including Australia, are that bariatric surgery is indicated in people with a body mass index (BMI, kg/m2) of greater than 40 or a BMI over 35 with serious health problems, such as type 2 diabetes.
These guidelines are based on those developed by the United States’ National Institute of Health (NIH) in 1991, when a different range of operations were available and surgery was not performed laparoscopically. Because of this, some researchers have recommended governments lower the threshold of eligibility to include people with a BMI over 30 without metabolic complications.

The reduction of the threshold may result in too many people having surgery inappropriately. While bariatric surgery is the most robust treatment for obesity, it is invasive, often irreversible and has associated risks.
Despite the proven efficacy of bariatric surgery, there is no way that it can be delivered on a mass scale. This surgery should be reserved for patients with severe obesity or patients with diabetes who have been compliant with treatment but have been resistant to medical treatments.
Furthermore, there are many new treatments in the pipeline that may mimic the beneficial effects of surgery, such as medications with effects on multiple hormone pathways and less invasive surgical procedures that may be as effective as the current operations with fewer complications.