

Like its Big Pharma peers, Gilead Sciences enjoys lavish taxpayer subsidies via the Pharmaceutical Benefits Scheme (PBS). It also makes large profits, but it pays little in the way of income tax in this country. So, like its peers, Gilead is doubly subsidised by Australian taxpayers: low income tax, high PBS.
Yet this US drug company has surpassed its peers in the pursuit of corporate welfare. It has set prices so high for Sofosbuvir, its “blockbuster” treatment for hepatitis C, that very few people in the world can afford to pay for the drug without monumental government subsidies.
Global Justice Now, a UK activist group, estimates somebody dies of hepatitis C every 79 seconds; in that time Gilead makes US$26,068 selling Sofosbuvir. More than 1.4 million people have died since Gilead took its hep C cure to market in 2014.
But what a cure it is. The success rate is 95%. Sufferers don’t need to take the drug for their whole life, just for a 12-week course of pills. This drug is capable of eradicating a disease that kills nearly 500,000 people a year and infects more than 150 million people worldwide … were it not for the money.
Only wealthy patients and wealthy countries like Australia have the wherewithal to pay for it. And Australia, with its “soft-touch” PBS scheme which is unsustainable and skewed heavily in favour of drug companies, is a prime target for Gilead.
The high cost of a cure
The Australian government forked out A$1 billion in just four months last year to subsidise hep C cures Ledipasvir and Sofosbuvir. These were the two most costly items on the PBS. This A$1 billion paid for just 43,000 prescriptions, prescriptions that would have cost the customer A$1,000 a pill had taxpayers not picked up the bill.
The extreme price of Gilead’s hep C cure led Dr John Freeman to set up a buyers’ club, FixHepC, so his patients could import a generic hep C treatment from Asia and pay $US2,000 rather than the $US84,000 Gilead was charging for the treatment in America.
Freeman’s son, Dr James Freeman, said this week he was apprehensive at first about importing a far cheaper generic from Asia but felt, as a doctor, he first owed a duty to heal his patients. It was the patients who imported the drug and the results were stunning, at a fraction of the price.
Patients of the Freemans were able get around patent laws on a personal use basis. Gilead, which has a 20-year IP stranglehold on the drug, is not happy about generic interlopers in its hep C market – though the company declined to respond to questions for this column.
A takeover windfall
The rationale for keeping drug prices high while allowing those who can’t afford to pay to die is primarily one of risk, capital and markets. Unless there is a significant financial reward for developing pharmaceuticals, companies will not invest and therefore cures will not be found. But where is the line to be drawn between profits and peoples’ lives?
James Freeman says, in the case of Gilead and its hep C drug, Gilead has overstepped that line. It didn’t develop the drugs, it acquired them in a takeover bid and then jacked up the prices.
Typically, a new drug costs between $US90 million and $US300 million to develop. Instead of developing the drug itself, Gilead acquired Nasdaq-listed stock Pharmasset for $US11 billion. It was framed as a “high-risk” acquisition at the time as Pharmasset had steered its drug through Phase II clinical trials but was yet to get approval from the US Food and Drug Administration.
“Patent laws are supposed to help incentivise research and development by ensuring profits for new drugs. But Gilead did not invent Sofosbuvir,” wrote Freeman in a paper on the hep C cure. “The research for the drug was partly funded by American taxpayers and the investment that Gilead made in buying the rights for the drug was more than made back in their first year of its sale. So most of the money you pay for the drug now goes to marketing and to paying dividends to the shareholders gathering in California right now.”
Gilead got Phase III trials done, had the drug approved, and the rest is history.
“In the third quarter of 2013, Gilead had US$2.36 billion in cash and convertibles on its balance sheet,” says James Freeman. “Now they have US$32 billion. They only have one blockbuster so they have US$30 billion in cash profit.”
Huge profits, little transparency
This sort of astronomical profit – a profit heavily subsidised by Australian taxpayers via the PBS – suggest Gilead should be accountable for its corporate activities in this country.
Like many Big Pharma multinationals that operate in Australia, however, Gilead produces only “Special Purpose” financial statements, a statutory report that relies on the assumption that there is only one stakeholder interested in Gilead’s financials.
This is wrong. It is a narrow and arguably erroneous view of accounting standards; creditors, taxpayers, patients, myriad parties are interested in Gilead’s financial statements.
The reason for producing Special Purpose reports is reduced disclosure, secrecy. There is zero disclosure, for instance, of Gilead’s related party transactions with its parent company in Ireland – likely there are IP or service charges to Ireland – or with the ultimate parent company in the US. The accounts fail to provide a “true and fair” picture of Gilead’s financial position as required by accounting standards and the Corporations Act.
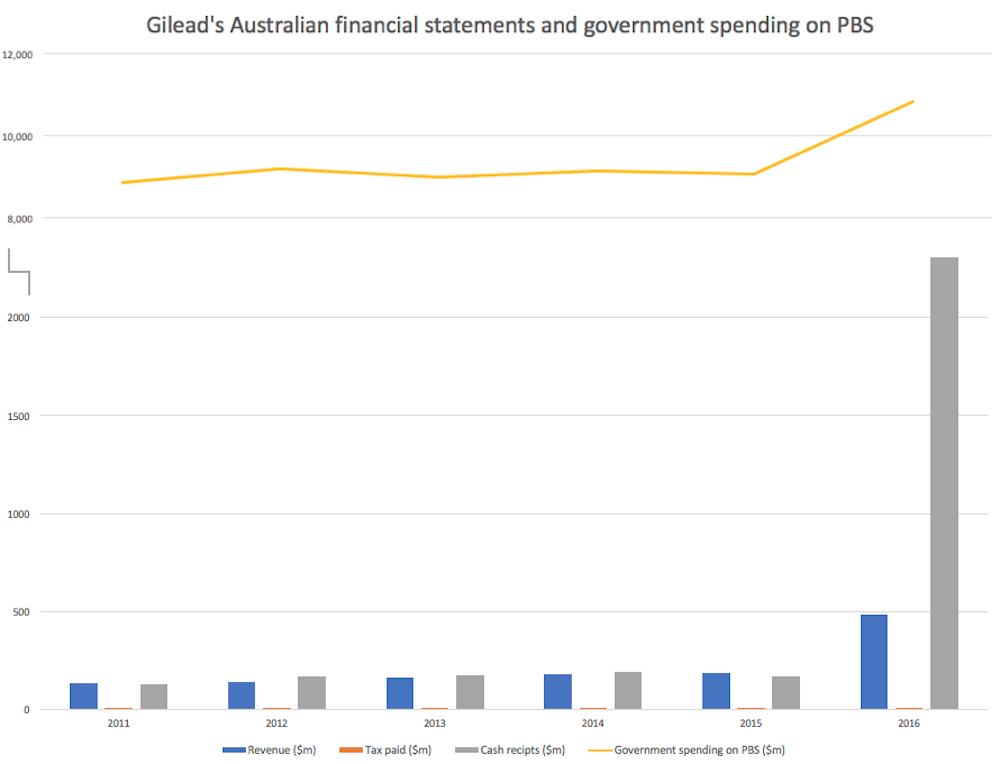
An analysis of its financial statements shows that although Gilead booked A$2.3 billion in cash receipts from its customers in Australia last year, it paid just A$2.8 million in income tax over the past six years. Tax as a percentage of revenue is 0.82% – less than 1% of sales – after billion-dollar subsidies via the PBS.
Further, deep in the intestines of the notes to the financial statements is a provision to pay the Department of Health A$1 billion. Never mind that this provision does not show up in “provisions” on the balance sheet – we have come to expect this sort of lousy accounting – but there is no explanation of the group’s arrangements with the government.
On the face of it, Gilead owes the government A$1 billion but does not deem that the government is entitled to an interest in its financial statements, ergo Special Purpose reporting.
Gilead’s revenue last year was A$483 million – it had soared from $186 million the year before – but it booked A$2.3 billion of cash receipts from Australian customers. How is it that cash of A$2.3 billion amounts to five times disclosed revenue? No doubt there are complex rebate arrangements, though these are not explained by Gilead or its auditor EY.
Neither is the government’s reporting of its PBS arrangements adequate. Again, cloaked in secrecy. The PBS spend has almost doubled in a decade from A$6 billion to A$11.5 billion and is headed higher. The long-term cost of health care appears crushing and a first step to averting this impending crisis in funding is transparency and disclosure.
As for Gilead’s social licence to operate in Australia, it hangs by a thread. This is a company that should be deemed an agent of its foreign parent and taxed as such.
The case of Gilead and Sofosbuvir is far from unique, says Dr James Freeman. “Across the world, hundreds of millions of people are priced out of accessing the medicines they need by big pharmaceutical companies with monopolies over essential medicines.
"It’s estimated that 10 million people across the global south died from AIDS-related diseases while big drug companies tried to block the production of ‘generic’ versions of drugs that could be used to cheaply treat patients. In the UK the annual NHS drug spending has gone up by £3.8 billion in the last five years and the NHS increasingly has to reject or ration new drugs because of their costs, leaving patients without access to new treatments.”
This column, co-published by The Conversation with michaelwest.com.au, is part of the Democracy Futures series, a joint global initiative between The Conversation and the Sydney Democracy Network. The project aims to stimulate fresh thinking about the many challenges facing democracies in the 21st century.