
Employees are the public hospital system’s most valuable resource, and its biggest cost. Wages account for nearly 70% of recurrent hospital spending. To keep hospital care affordable in a time of rising demand, it’s vital that skills are used to the full. Yet many professionals work well below their skill level.
Does it take 15 years of post-school medical education to safely do a colonoscopy or give light sedation to a stable patient? Does it take a three-year nursing degree to help someone eat? Trials in Australia and decades of experience overseas show that many roles performed by doctors and nurses can be undertaken by less highly-trained staff.
Yet as one Australian hospital CEO told us, fixing the mismatch between health workers and their work is “necessary and inevitable but seems to be taking forever”.
Grattan Institute’s new report, Unlocking skills in hospitals: more jobs, better care, shows how work can be reallocated to cut the cost of care without jeopardising quality and safety. It can also make the work of doctors, nurses and allied health professionals, such as physiotherapists and occupational therapists, far more fulfilling.
It’s important to do this now. As the population ages, demand for care will grow and the proportion of working-age people will shrink. Reserve Bank Governor Glenn Stevens recently highlighted these trends saying that in future,

…the question will be less “where will the jobs come from?” and more “where will the workers come from?”.
Alarmingly, Health Workforce Australia has predicted a shortage of 80,000 registered nurses by 2025.
At the same time, government budgets are under severe strain and hospital expenditure is growing faster than any other area. If we don’t increase hospital efficiency now, we could be stuck with much tougher decisions in the future, such as deciding who should go without care.
One solution our report proposes is to employ more nursing assistants. An Australian study found that nurses spend 3-9% of their time simply on patient hygiene and clerical work. Our survey of hospital CEOs suggests that nearly a third of nurses’ workload could be done by less qualified workers without reducing the safety and quality of care.
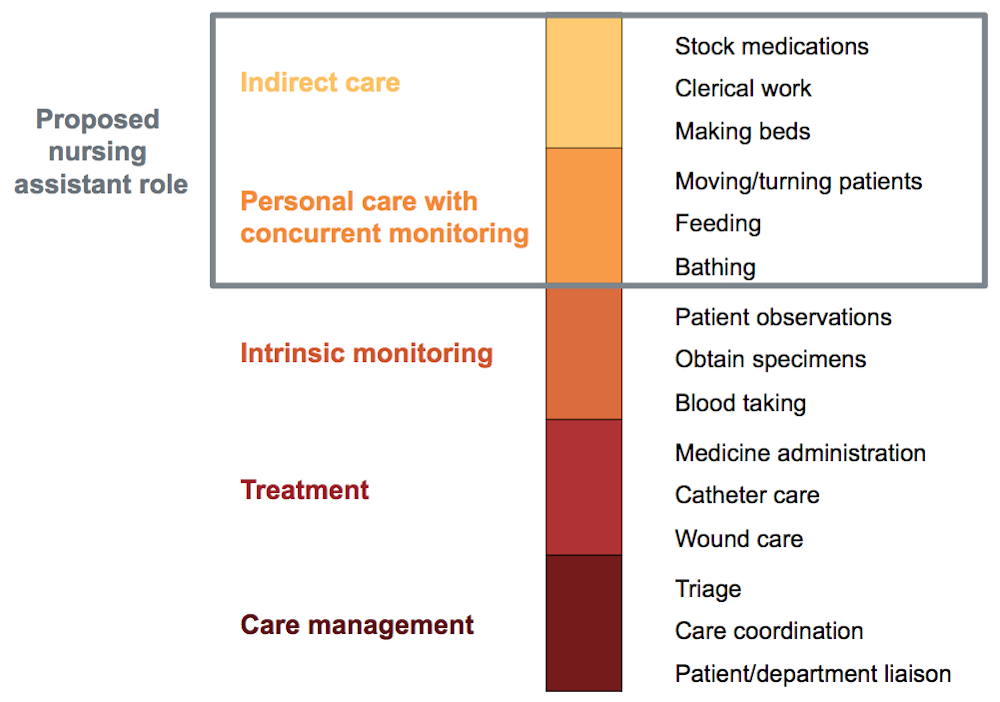
With a clear and limited role, and the right training and supervision, assistants could safely take on 15% of the current nurse workload. They would only provide indirect care, such as stocking supplies, and personal care, such as helping patients to dress, eat and bathe.
The change would give nurses more time to focus on urgent and complex work, making their jobs more manageable and rewarding.
Another example is enabling nurses to do some common, low-risk procedures that are currently only done by doctors. Many studies show that experienced nurses can readily learn to perform specific procedures well, safely and with high patient satisfaction.
In the United Kingdom, nurses perform around one in every seven endoscopies (looking inside the body through a tube). In the United States, nurses routinely deliver anaesthesia. Yet even though similar roles have been tried in Australia with good results, there are very few endoscopy or sedation nurses.
These two changes alone could save public hospitals A$390 million a year. The report also shows how using allied health assistants to take on work done by physiotherapists and occupational therapists would save another A$40 million a year.
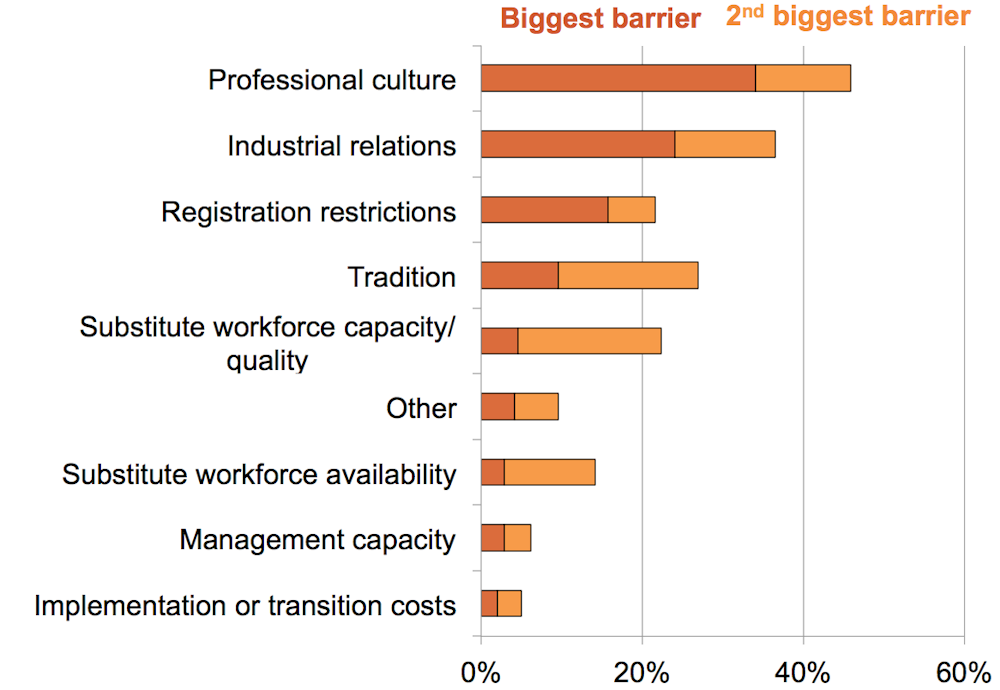
There’s no shortage of ideas about how to get a better match between hospital jobs and skills. There have also been plenty of pilots to test those ideas. The challenge is putting them into practice throughout the hospital system.
Rules and regulations are part of the problem. Some small changes to registration and training would help. For example, states will have to adjust legislation to let sedation nurses provide anaesthetic drugs, and there should be consistent national standards for nurse assistant training.
Industrial relations stalemates are another barrier. To unlock change, state governments could offer nurses access to new roles, such as sedation nurse, and at the same time guarantee no loss of jobs across the state. Because of strong growth in demand, these changes can happen through hiring, not firing.
To counteract inertia – a powerful force in the health system – states should give hospitals grants to fund the entire cost of new workforce groups such as endoscopy nurses, then taper down the grants over time. They should also offer training and support to help make sure the workforce changes are introduced properly.
These investments would be paid back through lower hospital costs just a few years after work is allocated more efficiently.
Our proposals are sure to raise hackles. Yet they are not radical. There is good evidence they are safe for patients – in some cases patients even prefer them to existing practice.
These changes don’t require wholesale reorganisation or creating new professions. They can generate new employment opportunities for lower-skilled workers, make professional jobs more rewarding and make hospitals more efficient. Updating workplace roles will meet resistance, but overcoming it should be an easy choice.