

Rwanda is located in the poorest region in the world, sub-Saharan Africa. Despite this, it is making advances with off-grid renewable energy solutions for rural areas that could be a model for similar economies.
Rwanda has harnessed its endowment with enormous, untapped renewable energy generation potential to address the problem of how to get energy into remote parts of the country.
The approach being taken accepts that extending the electricity grid to remote areas is fraught with problems. It is expensive, transport costs are high, and accessibility is difficult. In sub-Saharan Africa, grid-extension costs $23,000 per kilometre.
A project to get clinics in remote areas of Rwanda onto reliable sources of renewable energy has recently been stepped up a notch with the introduction of technology that smooths distribution.
Small-scale generation for remote areas
Off-grid electrical systems, where power is derived from renewable energy, have the potential in Rwanda for taking advantage of several types of small-scale generation.
This has become more feasible with the development of new technologies that have revolutionised the possibilities for making these systems highly resilient and economically sustainable. Examples include smart meters with wireless communication and sophisticated technology for fine-grained monitoring and control.
Rwanda is taking advantage of developments such as this to crack the problem of getting electricity to remote clinics.
Uninterrupted access to electricity is a key requirement for improving care in health facilities. But access to either grid or off-grid electricity is still one of the grand challenges for rural health centres in the region. One-quarter of health facilities are not connected to any source of electricity. On average, three-quarters of facilities have no reliable source of electricity. This leads to a poor health care service delivery.
83% of Rwanda’s population live in rural areas. This makes healthcare in these areas all the more important. And ensuring that healthcare centres have power is vital.
To overcome this obstacle decentralised power sources such as PV systems are becoming popular in rural areas because of their cost effectiveness compared to grid extensions. PV systems basically convert solar energy to direct current electricity using semi-conducting materials. But these have not proved adequate in matching supply with demand because:
Health centres operate on a first-come first-serve basis. If health centres continue to use connected electronic devices without proper management, the chances of blackouts will increase and patients will suffer.
Unused energy from fewer patients than expected also presents a problem as energy is wasted. Making batteries available to store energy can be a way to ensure less is wasted, help avoid shortages and manage excess demands. But this option is expensive.
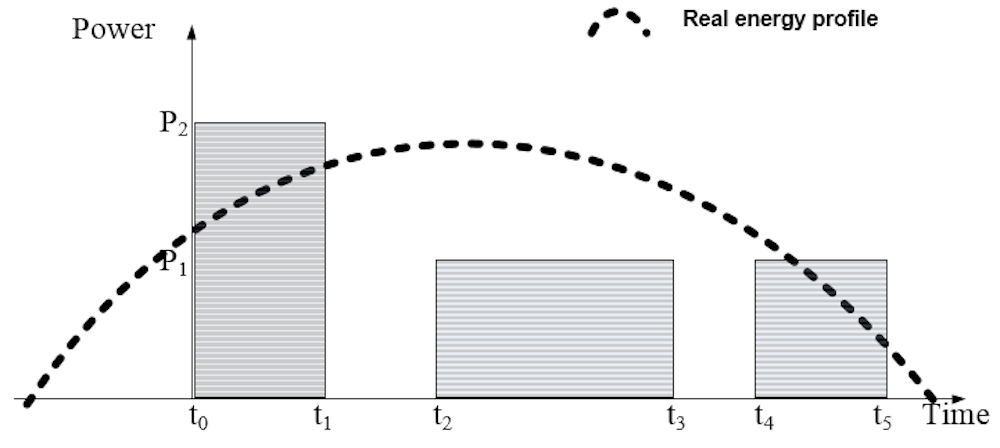
The graph below shows the ad-hoc scheduling of energy services in PV-power health clinics. Between t0-t1, the power demand exceeds available solar power. The t1-t2 window sees no load. This results in some services not being delivered, unnecessary use of batteries, and hence a shorter life-time, and less orderly operation.
Smart scheduling has done the trick
Smart scheduling is used to match consumption of active services with the available solar power. This results in minimum use of batteries or other energy sources.
The idea lying behind is as follows: the central controller estimates daily solar profile of the PV panels by pulling solar radiation information from online servers. Then when a physician wants to undertake an operation that requires electricity he sends a request to the central controller. This request includes power consumption and the duration of the operation.
In our prototype, the final decision lies with the system. Different services have different priorities. So, a surgery room may be given the highest priority during system planning. If an emergency occurs and a surgery room is fed into the system, it will be given the highest priority.
But human intervention is possible. The central controller is a photo voltaic (PV) inside the clinic. This means that a clinic administrator or the highest ranking physician can tap into the system, remove some services from the list and add some others.
The central controller checks the available solar power and the loads that are already being served. If there is sufficient excess energy, the request is confirmed and the energy is delivered. If there is not sufficient energy the controller schedules the request to when there will be enough energy. This may happen due to solar radiation, hence the generation, increasing or a service that was already receiving energy load being terminated.
In this way, facilities are used in a smart way and solar generation is used as it is generated.