



When deciding which treatments publicly funded healthcare systems should provide, medicines that extend terminally ill patients’ lives are among the most hotly debated – particularly for advanced cancer.
The National Health Service (NHS) spent an estimated £17 billion on medicines in England in 2016-17, roughly 13% of its budget. This was up from £13 billion in 2010-11, with the medicine bill currently increasing at over 5% a year as new drugs get ever more expensive.
Underlying this is a controversy many people probably aren’t aware of. The relevant authorities – the National Institute for Health and Care Excellence (NICE) in England and Wales, and the Scottish Medicines Consortium (SMC) north of the border – take a more generous approach to approving end of life drugs than all other drugs.
Yet according to our research, most people are not in favour. This raises searching questions about why it happened and what to do in future.
NICE numbers
NICE was first set up in 1999 (and SMC in 2001) to determine the availability of different drugs and treatments nationally, thus ending postcode prescribing.
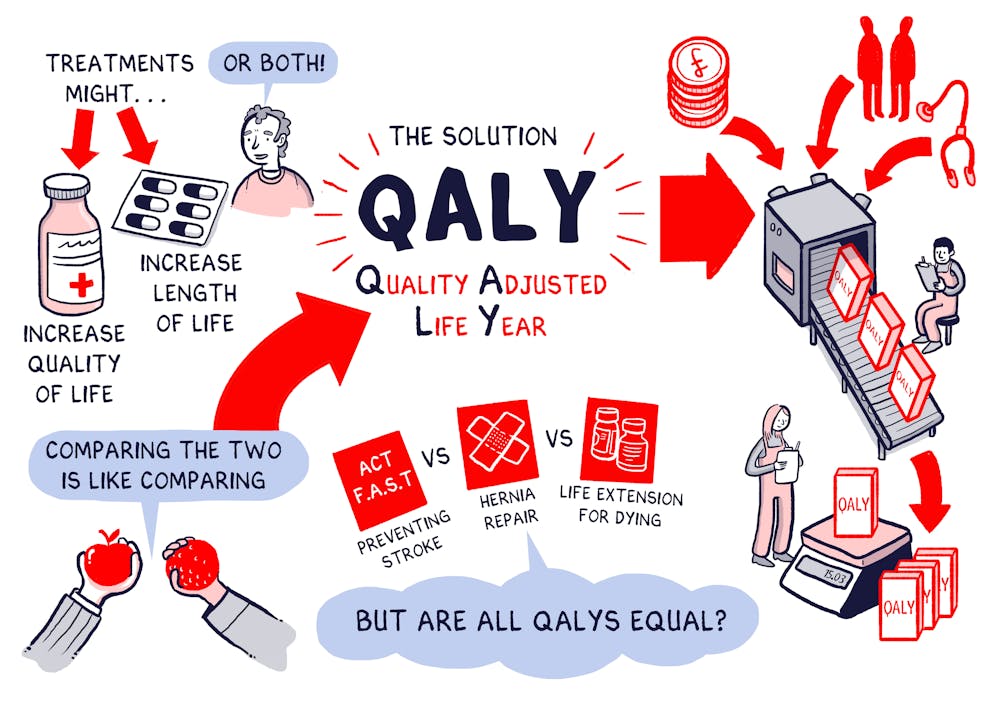
The two agencies decide which drugs to make available by looking at how many quality-adjusted life years or QALYs the average patient will gain from them. QALYs are calculated by multiplying how much a given treatment will lengthen a patient’s life by how much it will improve the quality.
You can then work out the “cost per QALY” by dividing the additional cost of the treatment by the number of QALYs gained. This is used to compare how much different treatments will improve patients’ health, per pound spent. For more explanation, watch this video:
When NICE and SMC were set up, they both introduced a threshold of £20,000-£30,000 per QALY, above which medicines are unlikely to be recommended. This presented problems for new end of life drugs, with their high prices and limited information about effectiveness.
The government was also under political pressure following media reports about cancer patients using life savings to buy drugs unavailable on the NHS. New Labour “cancer tsar” Mike Richards recommended making an exception to the general threshold. NICE duly introduced supplementary guidance in 2009, which set an effective threshold of £50,000 per QALY for medicines which extend life for at least three months.
In 2011, the Cameron government launched a special Cancer Drugs Fund (CDF) for England to enable still more patients to access cancer drugs not (or not yet) approved by NICE. The CDF’s cost per QALY threshold was estimated to be over £200,000 per QALY. The body was overhauled in 2016 because spending was getting out of hand, having spent a total of £1.3 billion on cancer drugs for 95,000 patients.
Nonetheless, QALYs gained through life extensions for terminally ill and cancer patients remain more highly valued than QALYs for everyone else – at least 1.7 times more. Senior figures at NICE and the CDF have justified this by claiming that the public places special value on extending lives. But does this stack up?
Public opinion
Previous studies show mixed results on public values in this context: eight out of 23 found that end of life health gains were valued more; 11 found the contrary, while another four were equivocal. This probably reflects differences in study design, but also suggests people are highly conflicted.

We sought to find out more. Where most studies focused on the choices respondents would make (for themselves or for society), we also looked at what people believed. We did this in three stages over a number of years.
First we sought the views of 59 specialists, including academics, clinicians, people working in the pharmaceutical industry, patient families and health policy makers; plus a sample of 250 members of the public.
They each had to arrange 49 statement cards on a grid, placing those they most agreed and disagreed with at either end. Examples were, “Treatments should be directed towards people who have a greater chance of survival”; and “We should support an individual patient’s choice for treatments that give short life extensions”.
Three viewpoints emerged:
- Viewpoint 1: Maximise health gain across the population to give best value for money overall, making no special case for end of life medicines. Many of the new cancer medicines therefore wouldn’t be provided;
- Viewpoint 2: Don’t deny treatments because of cost – prioritise patient rights and entitlements, not value for money. We should pay to extend lives, but all patient choice matters, not only terminally ill people;
- Viewpoint 3: Costs and benefits are key, as in viewpoint 1, but we should include non-health benefits like time to set your affairs in order. Sometimes even short life extensions are worth it, but it should be about quality of life and death, not extending life at all costs.
We then designed an online survey to test the prevalence of these views more widely. From nearly 5,000 respondents, 37% most agreed with viewpoint 1, 49% with viewpoint 2 and 9% with viewpoint 3 (the remaining 5% had mixed views). This mixed response echoes other population surveys.

Finally we asked 1,496 respondents to choose between policy options a national body like NICE must make, and treatment choices to reflect trade-off decisions made by regional health boards with fixed budgets.
Just 4% supported the options closest to NICE policy, and only 6% prioritised the equivalent treatment. Far more supported policies (32%) and treatments that improved quality of life (43% for end of life and 51% for non-terminal conditions).
What this means
Clearly NICE is out of step with public opinion – even if it’s not simple to make policy recommendations to reflect the views we found. When people did back paying more for end of life medicines, it was not to extend lives but to improve quality. This might imply shifting resources from expensive cancer drugs towards palliative and social care services.
The findings also raise questions about why the disparity between public and policy exists: is it government by headlines? Is it because industry lobbyists are being listened to instead? At the same time, if pharmaceutical companies made new medicines cheaper, these would meet the general QALY thresholds and none of this would matter. That key issue doesn’t receive enough attention from politicians or the media.
This much is clear: there is a gap between what the public thinks and the official approach to end of life medicines. We should recognise this and reflect on where we go from here.