

On 5th December last year doctors in public health facilities in Kenya went on strike setting off one of the longest and messiest industrial disputes by health workers in the country. The Conversation Africa’s Health Editor Joy Wanja Muraya asked Moses Masika to analyse the current impasse that’s paralysed public hospitals countrywide. _
What is the cause of the stalemate? How can the standoff be resolved?
Today marks 65 days of a standoff between government and doctors that’s deprived many Kenyans the inalienable right to quality health care and exposing many to extreme physical injuries and financial strain.
When doctors in Kenya began the strike two months ago they spelt out their demands clearly: they wanted a collective bargaining agreement signed in June 2013 to be implemented.
The government has chosen the wrong approach to end the strike. It’s attempted to coerce doctors to resume work by withholding salaries, issuing sacking letters and threatening to import foreign doctors from countries such as Cuba and India.
Union leaders have also been threatened with jail sentences for contempt of court.
These coercive machinations are intended to force doctors back to work. Instead they have strengthened their resolve. After so much sacrifice they feel there’s nothing more to lose.
The doctors’ resolve has also been strengthened by the fact that the government has refused to make any concessions, sticking to the same deal that the doctors’ union turned down in the first week of the strike.
What will get the doctors back to work?
The answer lies in implementing the 2013 Collective bargaining agreement.
It covers, among other things, fair working hours,improving work environments and equipment, training, research and remuneration.
Remuneration has been the most contentious. So far the government has offered an extra allowance but no basic salary increase. For any deal to stand a chance of ending the stalemate it needs to address all the issues, not just the addition of a solitary allowance.
The habit of using technicalities and bureaucratic red tape to frustrate the negotiations also needs to stop. And all stakeholders should be ready to come up with solutions rather than erecting roadblocks along the road to a deal.
Ultimately, the government needs to place the interests of the public first. It’s required to provide quality health care to all its citizens. Instead it is disregarding the needs of the majority of Kenyans who cannot afford private health care.
2. What effect has the strike had over the last two months?
Millions of Kenyans have been unable to access care in public hospitals.
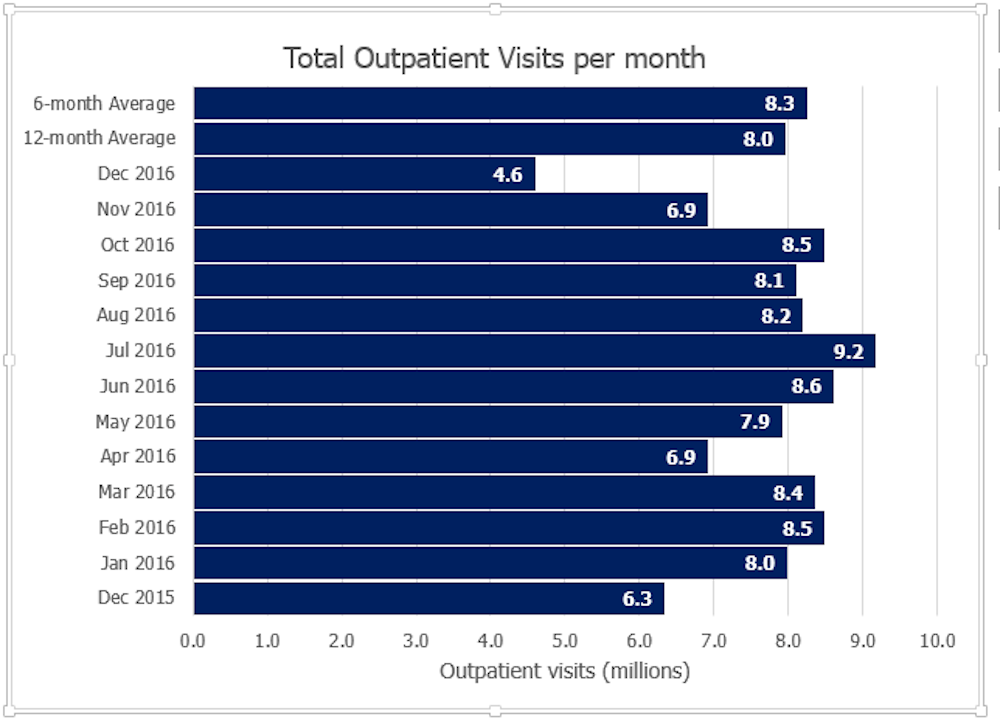
National data shows that the number of outpatient visits in December 2016 was about half of the average in the previous 6 months (Table 1).
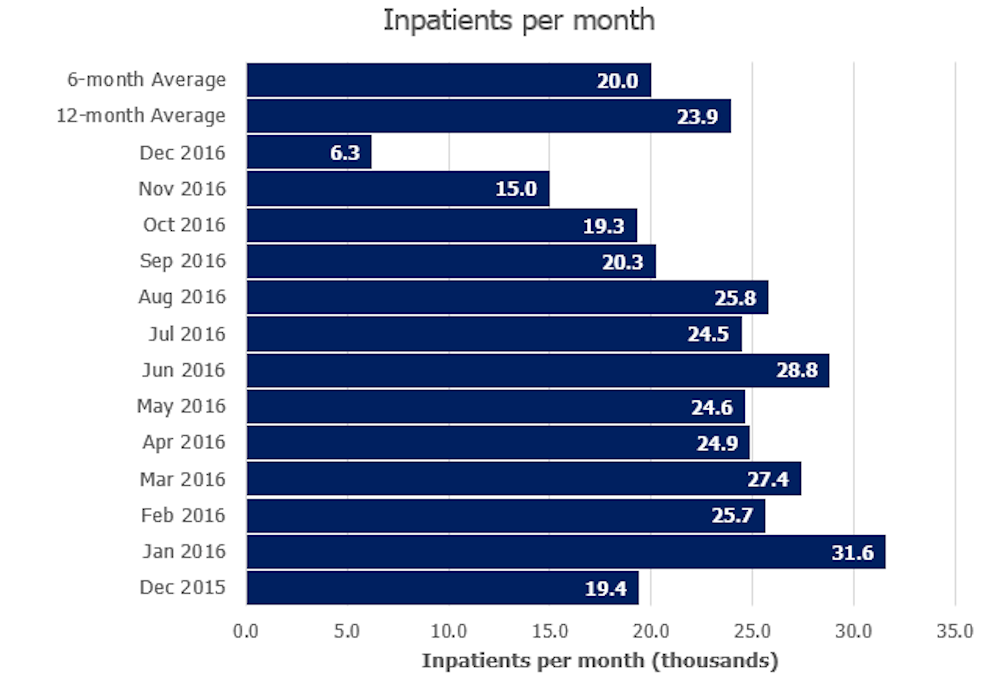
In addition, the number of inpatients per month has reduced to less than a third compared to previous months. This shows that millions of patients have not been able to access care in public facilities.
The most perturbing effect is that many patients have died or suffered disability because they could not access care. On top of this, many people have been forced to seek health care services from private hospitals, incurring catastrophic financial liability.
The strike has also led to delays in training schedules. University lecturers in all public medical schools across the country have been forced to stop teaching until teaching hospitals resume work. It’s impossible to teach medicine without patients in the hospitals.
This is likely to delay the release of new doctors who are supposed to graduate from medical schools this year, exacerbating the shortage of doctors across the country.
The strike has also placed heavy workloads on private and faith based health facilities which have had to contend with higher number of patients. This has stretched existing facilities and human resources, potentially reducing the quality of care.
3. Ethically, should doctors and nurses go on strike?
Doctors are bound by the Hippocratic oath not to harm patients under their care. That’s why, for instance, those who were performing surgery when the strike started didn’t abandon their patients but completed the operations first.
Secondly, the oath places special obligations on doctors towards their fellow human beings – whether they are ill or not – and charges them to take all the necessary measures to benefit the sick.
In the current strike, doctors have clearly outlined the benefits of their demands to the general public. If the government meets its obligations, there will be more doctors in public service and they will be better equipped, trained and motivated.
Therefore the burden of abandoning patients is not to be borne by the doctors: the government bears the responsibility to provide health care to the people. After all Kenyans pay their taxes to the government, not to the doctors, and should expect the government to provide essential services in return.
4. What needs to be done after the strike, to restore confidence in public health facilities?
Resolving the current strike positively would alleviate two major problems that bedevil Kenya’s public health facilities – the shortage of doctors and insufficient equipment.
That notwithstanding, the government will need to go further and address the problem of health care financing by making it equitable. Currently settling health bills impoverishes many Kenyans.
The National Hospital Insurance Fund has been expanded to cover many health care costs but the country still falls short of universal health coverage.
Kenya also needs to empower public hospitals to take advantage of the fund’s expanded coverage to grow and improve their services.
At the moment a disproportionately large chunk of the National Hospital Insurance Fund goes to private hospitals leaving public hospitals with constrained budgets. Public hospitals provide subsidised services and often fail to receive payment for services rendered.
This means that the hospitals cannot acquire the supplies or equipment they need to offer quality services.