

Australia has a relatively strong health system by international standards, but it needs a makeover. To generate fresh ideas, The Conversation is profiling five international health systems that have important lessons – good and bad – to pull Australia out of its health reform black hole.
Norway and Sweden remind us of a vision we have lost: the economic benefit of a strong, single national health insurer.
The economic case for a single payer health insurer is strong, but among prosperous countries there are few guiding examples. Many countries with strong public insurers have compromised that ideal by allowing or even encouraging (as is the case in Australia) private insurance to displace public funding.
Private insurance, however, is an expensive way to fund health care. When we look at the relationship between private insurance and a nation’s total health-care costs, we find a strong positive relationship: the more a country relies on private insurance the more it pays for health care, without any extra benefit.
It’s not just the bureaucratic cost of private insurance; it’s also the distortions it introduces, for when there is a private insurer in the market, able to pay premium prices for priority access to care, prices throughout the health system rise, both for the public insurer and for those who pay for health care from their own pockets.
The graph below shows the relationship between countries’ health-care costs (as a proportion of GDP) and reliance on private insurance. These are all countries with only minor differences in their health outcomes. (For the statisticians, R Squared = 0.66.)
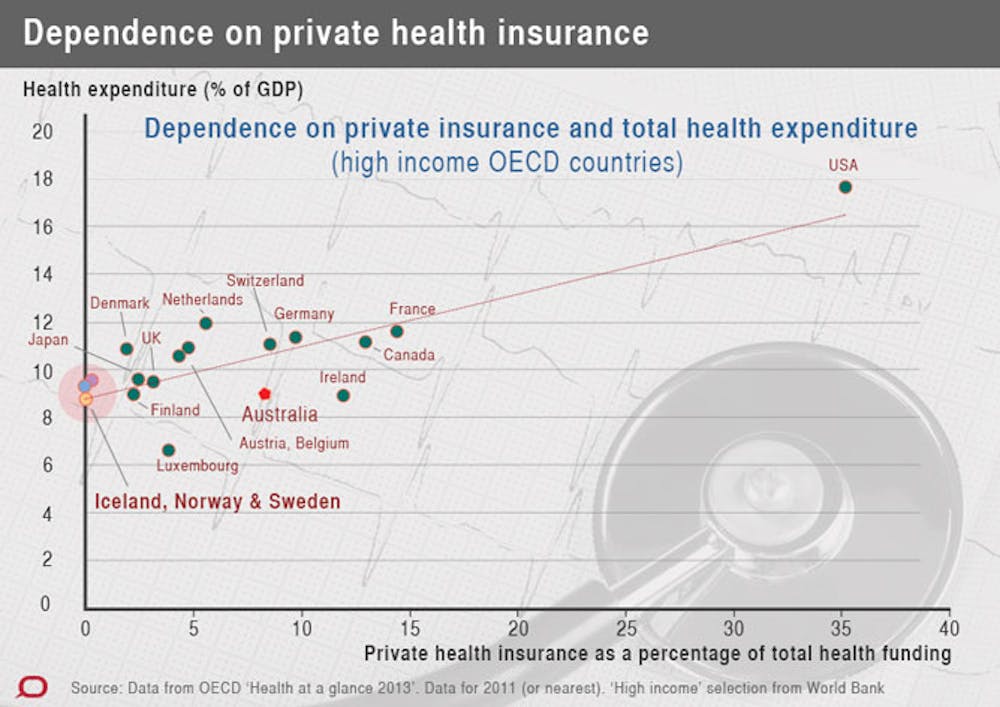
At one end of the scale, the United States stands out. At the other end are three countries – Sweden, Norway and Iceland, where private insurance is either absent or plays a minuscule role in funding health care. And these countries contain their total health-care costs (as does Australia for now), to around 9% of GDP. This is in spite of the fact that Sweden, the largest of these countries, has a significantly older population than Australia.
Click here to view our international health systems infographic
It is easy to conflate the notion of a single national insurer with that of “socialised medicine”, in which the state owns and controls all health-care resources, but that is not the case in these countries.
In Norway, almost all primary care is delivered by private doctors, while in Sweden there is mixed provision. In both countries patients can choose their doctor (Norwegians are encouraged financially to register with one GP of their choice), and there is a mix of salaried and fee-for-service payments for doctors.
Sweden’s primary care system makes good use of nurses, and its clinics generally include a range of specialist services. They are much closer to a “one-stop shop” than Australia’s suburban practices and GP superclinics, and more like the community health centres that thrived briefly in Victoria and the ACT in the 1970s.
In both Norway and Sweden, while most hospitals are government-owned, there are also private hospitals. But all hospitals, public and private, provide services to what we in Australia would call “public” patients. Unlike the situation in Australia, there is no social differentiation between private and public hospitals.
Another characteristic of both Norway and Sweden is subsidiarity. That is, the devolution of decision-making to local authorities. In Norway, the organisation of primary health care is the responsibility of its 428 municipalities, while in Sweden health care is devolved to 21 county councils.

In both countries, particularly Sweden, sub-national governments play a significant role in collecting taxes and funding health services. National funding provides compensation for regions with low means or high needs. But standards of care, negotiation with powerful providers (including pharmaceutical firms), approval of drugs, and levels of patient contributions are set by national governments.
In both Norway and Sweden, most patients contribute, from their own pockets, to the cost of health services. In Sweden, primary care visits involve out-of-pocket charges of SEK 100 to 320 (A$15 to $50). But there are exemptions for those with low means and total annual payments are capped at around SEK 4400 ($A700) for all services other than dental.
Norway has slightly higher co-payments, but a lower total safety net of NOK 2620 (A$460).
These figures may seem high to Australians, particularly when our political debate is focused on a possible A$7 co-payment, but they are in the context of prosperous countries with a much more egalitarian distribution of income, and much fairer tax systems. In fact, nationally, out-of-pocket costs are a little lower than in Australia – 15% of GDP in Norway and 17% in Sweden, compared with 20% in Australia.
An important difference with Australia is that in these Nordic countries, providers’ charges and out-of-pocket payments are set by government — a situation applying here only to prescription pharmaceuticals. This is in contrast to the haphazard and often inequitable imposition of out-of-pocket payments in our arrangements.
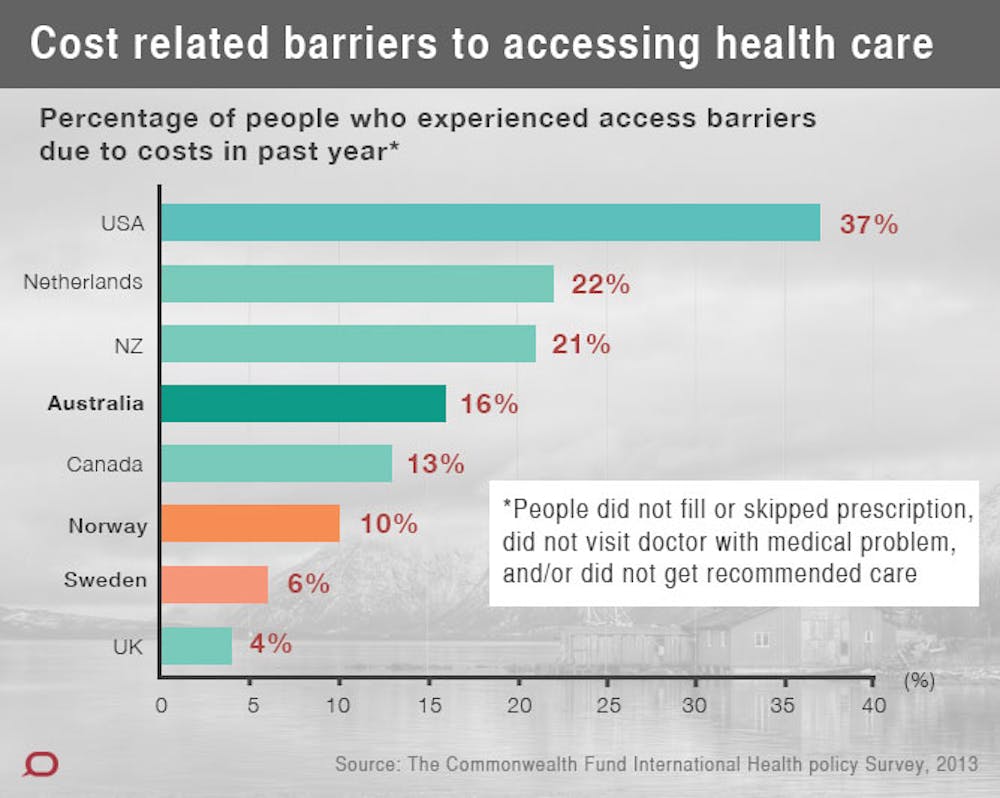
A survey in 2013 found that only 6% of Swedes and 10% of Norwegians reported cost-related access problems, compared with 16% of Australians. The same survey found that 25% of Australians spent more than US$1,000 on out-of-pocket costs, compared with 17% of Norwegians and just 2% of Swedes.
These figures contain a lesson for a government trying to insert a co-payment into Medicare, while ignoring overall efficiency and fairness in health funding and failing to engage with the community on health funding.
The main characteristic of these Nordic systems is a judicious mix of the single-payer national insurance and market signals through well-structured co-payments, without the distortion of private insurance.
Sweden’s centre-right Coalition Government, elected in 2010, has allowed firms to provide private insurance as part of employee benefits, with an aim to getting priority treatment. About 4% of Swedes are covered by these schemes but their contribution to spending is very small, because they cover a young and fit segment of the population.

If they do start to have an influence on health costs and accessibility Swedes will soon realise, as Australians do, that shifting some people to the front of the queue shifts others further back, while the cost of the distortion is widespread.
Whether this scheme survives may depend on the outcome of the Swedish election on 14 September. Opinion polls are pointing strongly towards Swedes’ rejection of the current government’s policies in health and education, and a return to a government dominated by the Social Democrats.
It is hard to imagine these countries, held together by strong norms of egalitarianism and decency, heading down the path of social exclusion that Australia has taken in health care.
This article is part four of The Conversation’s International Health Systems series. Click on the links below to read the other instalments.
- What can we learn from other countries’ health systems?
- Creating a better health system: lessons from the Netherlands
- Creating a better health system: lessons from England
- Creating a better health system: lessons from Singapore
- Creating a better health system: lessons from America
- Infographic: comparing international health systems
- Australian health care: where do we stand internationally?