

When the movement to promote evidence-based healthcare began in the late 1980s, it started in the field of child birth. So it might be expected that by now, nearly a quarter of a century later, there would be consensus and consistency between countries about how care is offered. But this is far from the case, as data from the second Euro-Peristat report, Europe’s largest study of childbirth and maternal care, showed when it was published earlier this year.
Collaborators from 29 European countries, 26 in the EU plus Iceland, Switzerland and Norway, contributed official aggregated national data for the year 2010. The data was comparable because it used predefined indicators to compare births and maternity care in these countries. We were also able to compare changes since 2004, when figures were collected for the first report.
Who gets caesareans?
A key indicator was how babies were delivered, in particular the proportion of babies born by caesarean section. In situations where there are clinical complications, caesareans can be life saving for mothers and their babies. On the other hand, as caesareans can lead to longer recovery times and risks including complications in subsequent pregnancies, it’s important to avoid doing them when they aren’t necessary.
The report showed wide differences between caesarean section rates, ranging from 14.8% in Iceland to 52.2% in Cyprus. The other Nordic countries and the Netherlands had rates of around 17% while Poland, Romania and Italy had rates ranging from 36% to 38%. The rates for the rest of the participating countries came between these extremes. This included the UK, which had caesarean section rates of 24.6% in England, 26.1% in Wales, 27.8% in Scotland and 29.9% in Northern Ireland.
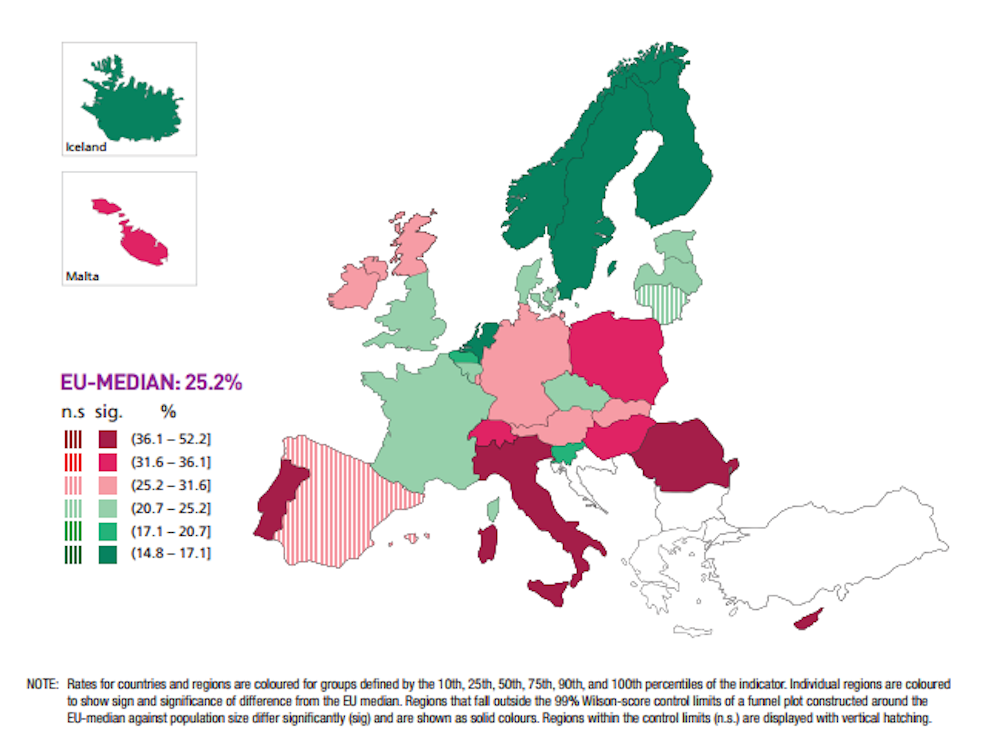
Why do rates differ so much between countries? Populations differ and older women, women having their first baby, women carrying babies in the breech position and women with multiple births are more likely to have caesareans. But these differences aren’t big enough to explain the sometimes very wide differences between countries – for example, nearly 40% between Iceland and Cyprus. Nor did countries with higher caesarean rates necessarily have lower proportions of babies born using forceps or vacuum extraction. The use of these was very low, mainly less 2%, in Eastern Europe and more than 10% in other parts of Europe which still vary in their rates of caesarean section.
And caesarean section rates also differ between maternity units within the same country. A study comparing this in France, where there is a substantial proportion of private hospitals, found they had higher caesarean rates than public hospitals after taking account of differences in the women delivering in them.
Higher rates have also been found in private hospitals in other countries. The UK has a very small private sector, with just two hospitals with private maternity units in England. One, the Portland cites a caesarean section rate of 51%, twice the national average, on its website. The other, the Lindo Wing, part of St Mary’s hospital in Paddington, west London, and popular with the royal family (although the Duchess of Cambridge recently opted for a natural ten-and-a-half-hours labour there), doesn’t publish the number of caesarean procedures it carries out or its rate.

Local differences
Other factors can also influence differences. NHS maternity units in England should all follow a common set of guidelines published by the National Institute for Clinical Excellence (Nice), which stipulates among many other things, that women should not be automatically offered caesarean sections which are not clinically necessary.
Despite this, in the financial year 2011-12, caesarean rates ranged from 15% in Shrewsbury to 33% in University College London, Barnet and Chelsea and Westminster Hospitals. Analyses of the data by London School of Hygiene and Tropical Medicine showed that even after the caesareans were broken down into subcategories and statistically adjusted to take account of mothers’ characteristics and clinical factors, wide differences persisted. This suggests a lack of consensus by clinicians about good practice within the same healthcare system.
Comparisons in the report between the 2010 figures and data from 2004 showed that caesarean section rates increased in most countries, with the exception of Finland and Sweden where they declined slightly. Increases ranged from under 0.2% in Italy to over 7% in Lithuania, Slovakia, and Poland. In general, these increases were most marked in the countries of Central and Eastern Europe and in Germany and Austria. And this is in accord with OECD data that shows rising rates in a range of middle and high-income countries.
The report is based on routinely collected data, so didn’t attempt to collect information about the reasons behind rate increases. But it did mention those that have arisen in other studies. These include a variety of reasons from women requesting caesarean births and the perception that caesarean section is an entirely safe procedure, to fear of litigation and financial incentives. As a WHO report also suggested the role of supply, demand and control. A recent Birthplace in England Research Programme also showed that midwife-led care is associated with lower intervention rates and it could be that midwives play a more prominent role in the Nordic countries and thus keep rates down.
Hard Evidence is a series of articles in which academics use research evidence to tackle the trickiest public policy questions.