

More than 600 nurses worldwide have died from COVID-19 during the pandemic. This should not be a surprise: we are the largest group of healthcare workers in the world, dedicated to preventing the spread of coronavirus, and we are also engaged in caring for those who are suffering.
But although we are on the frontline of this crisis, nurses are too often being left out of responses to the pandemic.
Uniquely at risk
In the UK and other countries with high rates of coronavirus deaths, there are increasing inequalities in health outcomes for different income groups. In England and Wales, the mortality rates from COVID-19 in the most deprived areas are more than double the least deprived.
In general, the risk of ill health increases for people who live on a low income. Common health issues that affect these groups include high blood pressure, coronary heart disease, lung disease, type 2 diabetes and obesity. All of these put people at higher risk of becoming sicker and dying from COVID-19. Death rates are highest among people from Black, Asian and minority ethnic backgrounds.
These communities are also disproportionately represented among nursing staff some of whom are living on the lowest wages.
Lacking equipment
Nurses working in hospitals, care homes and within communities are often put at greater risk from COVID-19 because they have not been given adequate personal protective equipment, or PPE.
A study of nearly 100,000 health workers in the UK and US found that people working on the frontline of the coronavirus pandemic were three times more likely to test positive for the disease than the general community. Health workers from a Black, Asian or minority ethnic background were found to be five times more likely to test positive than white people who did not work in healthcare. Workers who reported a lack of adequate PPE in their healthcare institutions were at greater risk still.
Another study by the UK’s Royal College of Nursing, meanwhile, found that more than half of Black, Asian and minority ethnic respondents have felt pressure to work without the correct PPE compared to just over a third of other respondents. These groups were also asked to reuse PPE more frequently than their white counterparts.
Denied a voice
It’s a painful irony that as nurses battle against the coronavirus pandemic, 2020 is the World Health Organization’s Year of the Nurse and Midwife which was supposed to raise the profile and perceptions of nurses globally.
But the response to the pandemic in the UK has starkly shown that our expertise and experience as a profession is not being called upon and our potential is not recognised. We are the biggest work force for health in the UK working in hospitals, care homes and community settings to care for those with COVID-19 and help prevent its spread yet we have no representation on the official scientific advisory group (SAGE), which advises the government on its coronavirus response. Nor are we represented on the rival Independent SAGE group.
Our role in policy development and planning is negligible despite the invaluable insights our unique position in health systems gives us. Our lack of representation and reward means that we are also suffering from the impacts of inequalities along with those we care for.

Given the chance, nurses could help guide coronavirus policy in a number of ways. First, by being a witness to the health impacts of COVID-19 on our local communities and staff, recording and researching inequity of access to services. Second, we can advise on how to provide prevention and treatment resources to those most at risk. Finally, we can set a positive example in terms of equality of opportunity, fair working conditions, protection from infection and pay. This could start with ensuring equal provision of PPE for all staff.
Nurses are at the forefront of trying to reduce existing health inequalities which are being made worse by COVID-19. We are also victims of those inequalities – a feminised, racialised workforce dealing with poor conditions and lacking a political voice. Care and prevention of disease are not perceived as being as important as finding a cure or a vaccine, but in the global recovery from COVID-19, all these elements are equally vital.
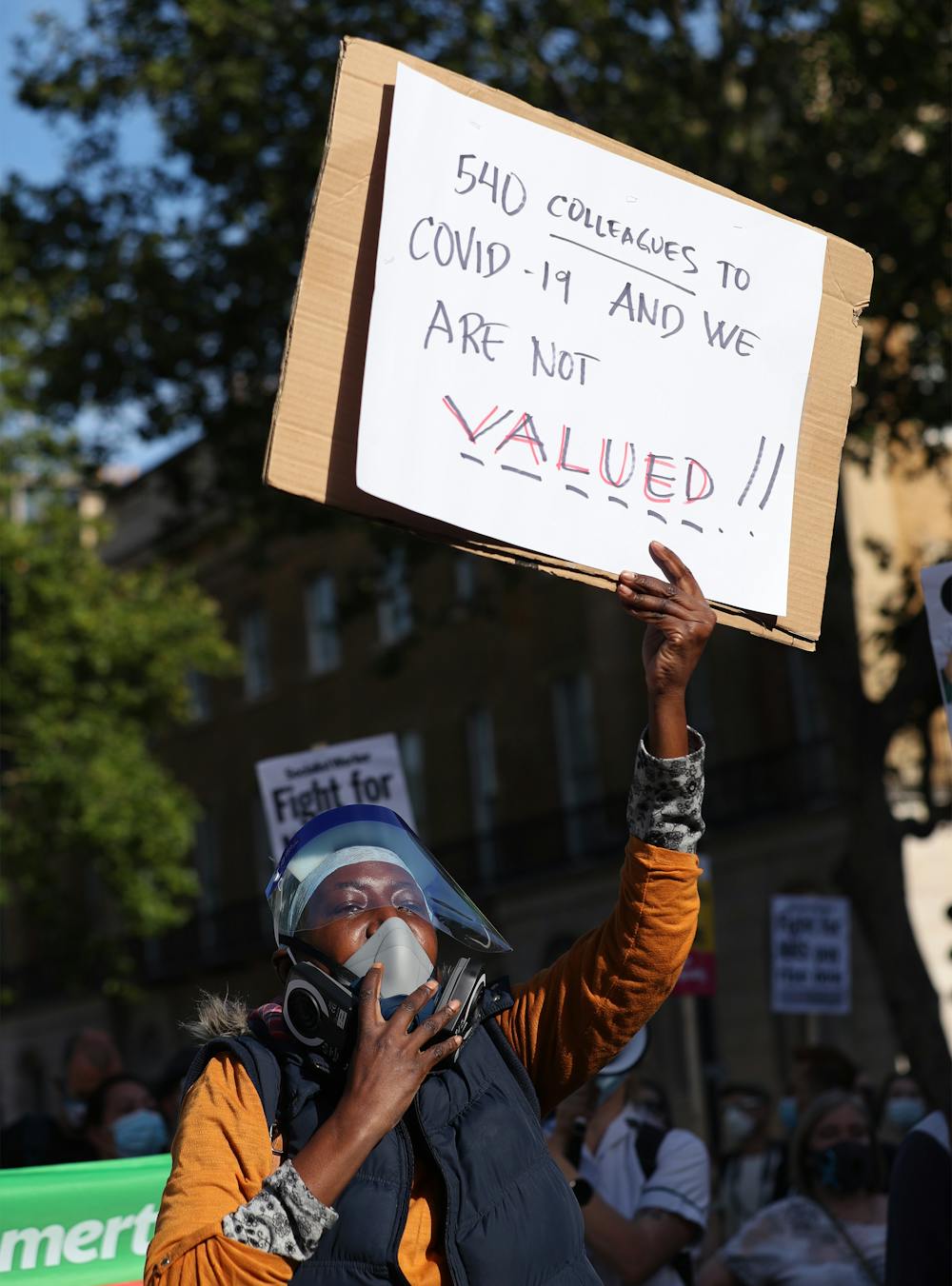
We have already lost too many colleagues in the fight against this disease. It’s time our work is recognised and we are given an official voice to help us all recover from the coronavirus pandemic.