

{kind=link}
Any analysis worth its salt of what it means to be poor will include indicators explicitly linked to health – nutrition, for example, or mortality rates. But in reality, the many different aspects of poverty are inextricably intertwined, and there are no indicators which do not imply an adverse effect of one sort or another on the physical or mental health of the person experiencing them.
Research we have just published on the multi-dimensional nature of poverty in 49 countries found that half the poor were so deprived they should be classed as “destitute”. What does it mean to live in destitution? Well, 41% of the destitute live in a household in which at least one woman or man has lost two or more children, 67% have someone at home with severe malnutrition, and 40% either don’t have clean water, or must walk a round trip of 45 minutes just to get it. In addition, 69% possess no assets whatsoever – not so much as a mobile phone or radio – and almost all cook with wood, dung or straw.
One of the most striking findings in our research was that a massive 90% of the destitute – 574.2m in these 49 countries alone – practise open defecation to relieve themselves. This has a huge health impact.
Public health and women’s safety
The UN puts the global number of people who openly defecated in public at 1 billion and according to the World Health Organisation, societies that practise open defecation are at risk from cholera, diarrhoea, dysentery, hepatitis A and typhoid, and tend to have the highest numbers of deaths of children.
The risks associated with open defecation are not purely from disease; besides the feelings of shame and humiliation that accompany squatting in a gutter or bush, there may be an entirely justified sense of fear and vulnerability. The lack of sanitation in rural areas has been flagged up by campaigners as a serious risk to women’s security as well as their health, as they are often attacked when having to go out, and particularly at night. The two teenage girls who were gang-raped and hung in a horrific attack in Uttar Pradesh in India in May had apparently gone out to relieve themselves as they had no toilet at home.
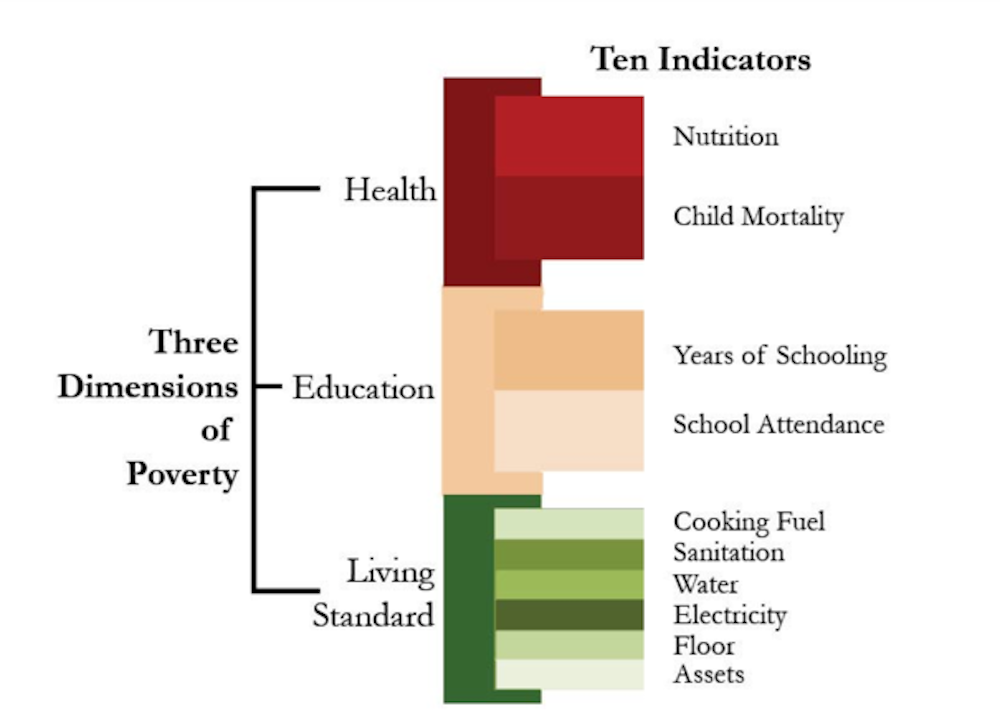
Sanitation is just one of ten indicators of health, education and living standards that are measured directly by the Global Multidimensional Poverty Index (MPI) in order to identify the poor and destitute. The Global MPI is the first international measure to reflect not only the incidence of poverty (the percentage of the population who are poor), but also its intensity – the share of overlapping deprivations each person faces at the same time. Other indicators include years of schooling, child mortality, nutrition and safe drinking water.
The index identifies a person as “poor” if they are deprived in at least one third of the ten weighted indicators. These same indicators apply to someone who is destitute, but according to more extreme criteria. For example, a person whose household includes someone who is malnourished is identified as poor, while a person whose household includes someone who is severely undernourished is considered destitute.
Changing picture
Despite the situation improving for many as a result of poverty reduction programmes and economic growth, there is still a formidable core of extremely poor people. Across south Asia there are 420m people living in destitution. India alone is home to 343.5m destitute people; more than a quarter of its population. However, of the 49 countries in the study, those with the highest share of destitute people are to be found in Sub-Saharan Africa. In Niger, a staggering 68.8% of the population is destitute.

Take Bibi Ayesha, for example, who lives in a box-like structure on stilts near a temple in Delhi, India. Injured in an accident years ago, she’s unable to walk and gets around on a hand-pedalled tricycle. For sanitation she relies on government restrooms near her makeshift home, which has no electricity or water and she earns a little money by cleaning a nearby homeless shelter and collecting alms in front of the temple. Most of the money is spent on medication for her chronic respiratory condition. What little food she can afford, she cooks over wood on a little mud stove and shares with her mentally ill son.
The good news is that where data is available, we can see strong progress being made to improve the lives of the destitute, particularly in the poorest countries. Of 34 countries for which there are data, the largest reductions in destitution were seen in Ethiopia, followed by Niger, Ghana, Bolivia, Rwanda, Tanzania, Nepal, Haiti, Bangladesh and Zambia; all of them are considered low income or least developed countries, except Ghana and Bolivia.

Our study found that in Ethiopia, the share of destitute people was reduced by 30 percentage points between 2000 and 2011.
Interestingly, in terms of indicators, the majority of these 34 countries registered significant improvements in sanitation and child mortality, suggesting that health and sanitation policies are playing an important role in improving the lives of the poorest of the poor.
Indeed, the success in tackling destitution seen in some of the world’s poorest countries sparks hope that progress is being made, and that concerted efforts after 2015 – the target year for the Millenium Development Goals – really can result in there being “no one left behind”. For now though, destitution – with all the grinding hardship it entails – continues to take a grim toll on the physical and mental health of hundreds of millions of people.