

Our new series, the Science of Medical Imaging, examines the technology behind non-invasive methods of creating images of the human body. In this first instalment, we look at two types of emission imaging: positron emission tomography (PET) and single-photon emission computerised tomography (SPECT).
As its name suggests, emission imaging works by detecting radiation emitted from within the patient, enabling clinicians to determine the presence and size of cancerous tumours, and conduct other diagnostic procedures such as coronary perfusion.
Hospitals use two main forms of emission imaging:
Both work on the same basic principles - detecting gamma rays and building a three-dimensional picture of, say, a cancerous tumour.

The basics of emission imaging
A radioactive tracer (radiotracer) is injected into the patient. Radiotracers are molecules such as glucose with a radioactive isotope attached.
As tumour cells rapidly grow, compared to neighbouring cells, they require large amounts of glucose. Blood carries glucose throughout the patient but it is absorbed mostly at the tumour site, carrying the isotope with it.
The isotope then decays, emitting gamma rays (photons that are much higher in energy than visible light and can pass out of the body). By collecting the gamma rays in detectors placed around the patient, we can build up a picture of where they came from, locating the tumour position and shape.
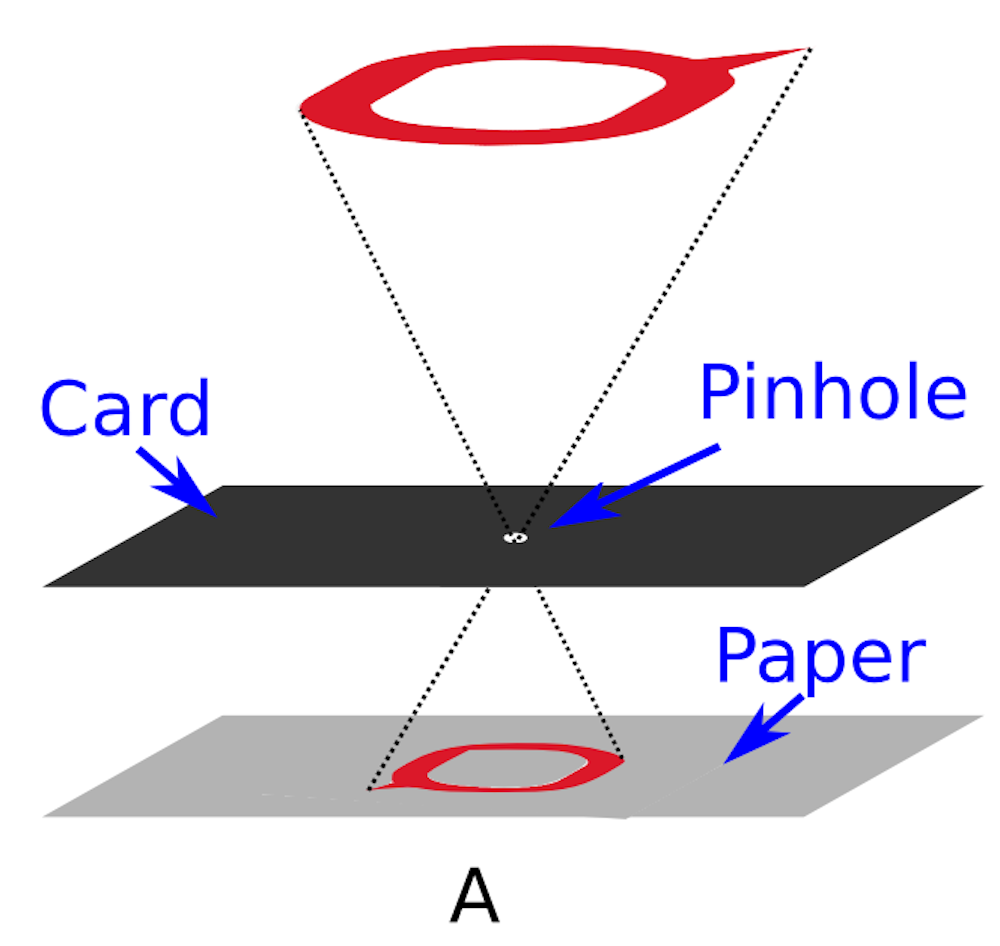
Many different detector systems are available. The simplest is the pinhole camera, which you may have used to observe an eclipse.
To do this, you prick a tiny hole in a sheet of card and place a sheet of paper behind it. A projected image of the eclipse is cast onto the paper. The projection appears back to front and upside down and is viewable without damaging your eyes.
This is shown in Figure A above; but the eclipse has been replaced with The Conversation logo. In the subsequent figures, our theoretical tumour is also replaced by the logo.
And while pinhole cameras are handy for eclipses, the simple design will not suffice for imaging in an oncology department.
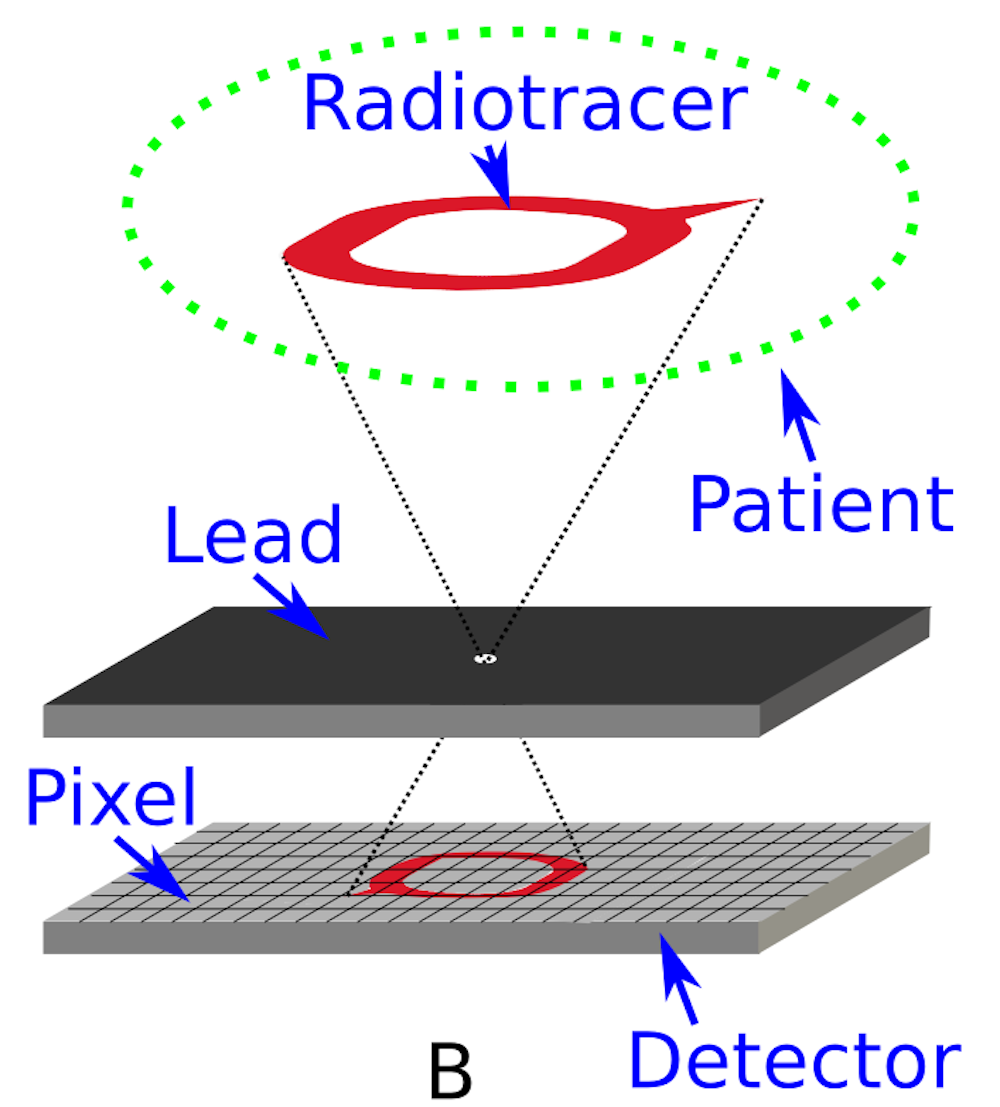
In this instance, the sheet of card is replaced with a sheet of dense metal (typically lead, and called a collimator) and the paper is replaced by a detector divided into pixels that can measure the position and energy of each photon that passes through the pinhole as shown in Figure B.
The detector is divided into pixels by the manufacturing process. The smaller the pixels, the more precisely we will know the location of where the gamma ray interacted.
The gamma rays emitted from the decay of the radioisotope leave the tumour in all directions. In Figure B, the two diagonal lines show the limits of the directions that they must follow to pass through the pinhole and interact in the detector.
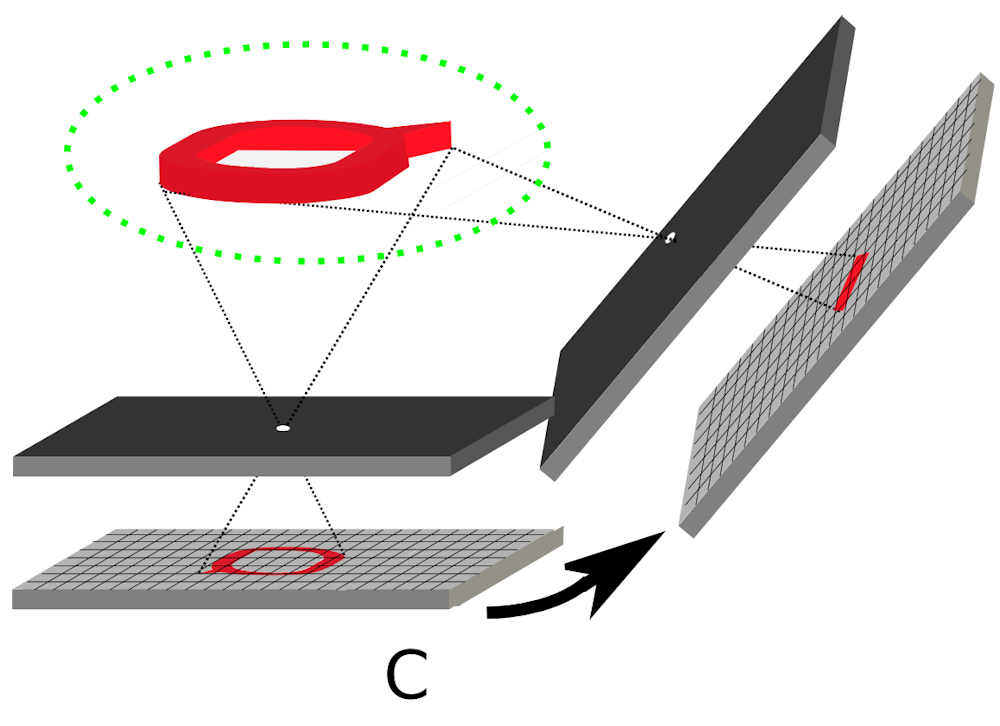
The tumour has a 3D distribution and the detector must be rotated around the patient - see Figure C above - to collect a projection at each angle as is performed in a SPECT scan in a hospital.
Putting it all together
After the radiotracer has “washed through” the patient, the aim of the exercise is to build up a picture of the tumour from a series of measured counts in detector pixels. We can’t simply add the counts in the detector at each angle - we have to perform a reconstruction.
For SPECT and PET this requires tracing lines back from the detector pixel to where the photons came from (inside the tumour). We do this for each pixel that records energy from a gamma ray.
We know we need two points to form a line. In SPECT, the two points forming each line are the pixel location and the pinhole location.
In order to increase the sensitivity of the device, we can punch more holes in the collimator, which will allow more gamma rays through. This means we can give the patient a lower dose of radiotracer, reducing the risk of causing secondary tumours by the very act of administering the radiotracer in the first place.
Differences between SPECT and PET
To demonstrate why SPECT and PET have different types of detectors, first we must understand the difference in radioisotope that is administered to the patient.
Figure D (below) shows two cartoon representations of a patient with a tumour that has absorbed the SPECT radiotracer (on the left) and the PET radiotracer (on the right).
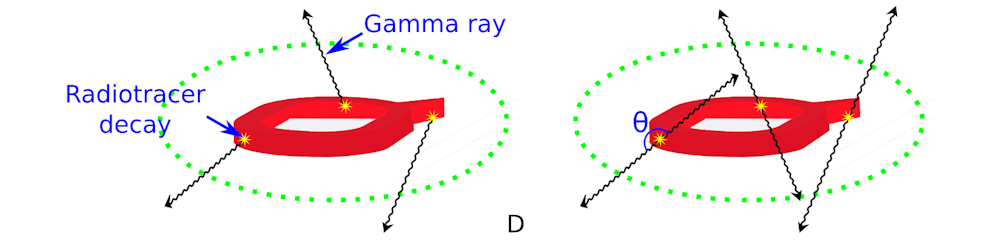
For both cartoons we have shown three of the millions of decays of the radiotracer that happen while it is inside the patient. For the SPECT case, the nuclear decay is straightforward and we get three gamma rays.
For the PET case, an intermediate positronium is formed, resulting in two gamma rays at each of the three decay sites, giving a total of six gamma rays.
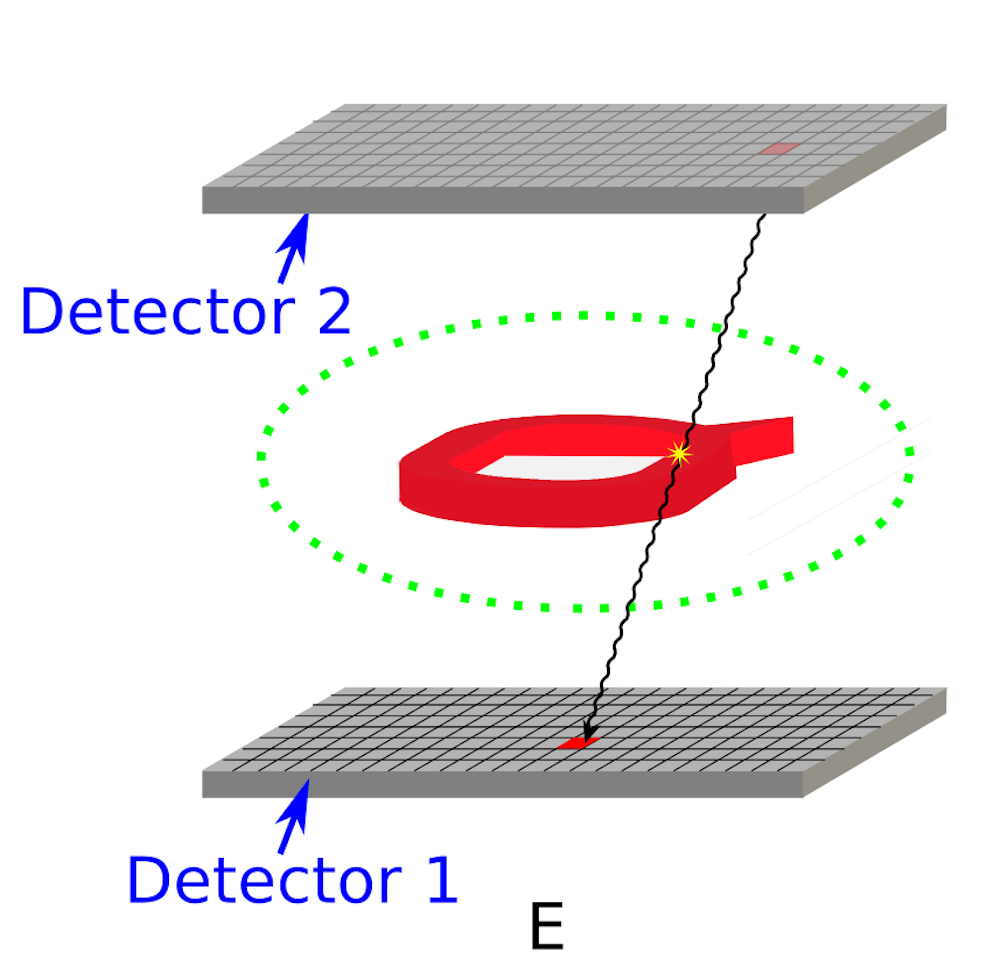
The great thing about PET radioisotopes is that each pair of gamma rays are primarily emitted at 180 degrees to each other. Figure E shows why this is so useful.
As mentioned already, the two points that form the line in the reconstruction in SPECT are the pinhole in the collimator and the pixel of the detector.
For PET radioisotopes, all we have to do is detect the two gamma rays for each decay and this enables us to trace the line that finds where the emission came from.
We can do this by including a second detector and throwing away the collimator, which means we get an enormous gain in sensitivity (up to 1,000 times).
Generally, SPECT radiotracers last longer in the patient and are primarily used in cardiology where myocardial stress imaging takes about three to four hours, whereas PET radiotracers emit gamma rays with shorter lives and higher energies and are more useful in brain imaging where scans last about 30 minutes.
As with everything in science, no system is perfect. PET does suffer from several resolution limitations and there are issues with the range of radioisotopes that decay via positron emission.
But they are two useful tools in the clinician’s arsenal for diagnosing disease in patients.
Further reading:
X-rays and CT scans
MRI