


For decades, clinicians and researchers have been concerned about patients getting treatments, including operations, that don’t work. As well as failing to treat the original health problem, ineffective care exposes patients to complications and side-effects and waste precious health-care resources.
Yet while many clinicians believe there is a problem, the policy response has been limited. It is often hard to isolate treatment choices that are inappropriate. A choice that is wrong in one case may be right in another.
To avoid ineffective treatments, we need a new way to identify and reduce questionable care. A new Grattan Institute report shows how to do it.
Warning signs
The report follows up two clues that treatment choices are sometimes wrong.
The first is geographic variation. In 2010-11, there were 1.3 tonsillectomies for every 1,000 people in Western Sydney. Along the Great South Coast in Victoria (the area around Warrnambool), the rate is 7.4 (these rates are adjusted for age and sex). It seems unlikely that variation this large is just a matter or people in some areas being sicker or more willing to go under the knife.
But while geographic variation is troubling, it is inconclusive. Some of it can be explained by factors such as how sick people are, but not all of it.
It is also hard to tell if over-servicing or under-servicing is the problem. Are people in areas with high rates of surgery getting too much, or are people elsewhere getting too little?
Finally, variation is typically measured among regions. That can make it hard to tell which providers are behind it. For all these reasons, years of debate and commentary about clinical variation has resulted in little policy action.

The second clue that alerts us questionable care is the use of treatments we know are ineffective for certain types of patients. Clinical research has uncovered hundreds of treatments that don’t work for certain types of patients. These treatments have been targeted for reduction or removal. Australian medical colleges have recently listed treatments that should be questioned in discussions between doctors and their patients.
Like clinical variation, ineffective care has been widely discussed but still persists. It is very hard to find treatments that are always wrong and efforts to shift treatment choices are sometimes met with indifference, resistance or gaming.
For instance, powerful evidence shows that a certain type of arthroscopy – inserting a tube to remove tissue – won’t help people with knee osteoarthritis. But it still happens at least 800 times a year in Australian hospitals.
What should be done?
The first step to address the problem is to provide better information. Clinicians cannot keep track of all the evidence published each year. Much of the guidance that summarise the evidence is flawed. We recommend that a body such as the Australian Commission on Safety and Quality in Health Care develop and publish clear guidance about which procedures should be avoided.
The second step is to monitor whether this guidance translates into practice. To show how this can be done, we measured how often hospitals provide five examples of do-not-do treatments. They are treatments that evidence, and usually government bodies, say should not be given to certain types of patient:
Vertebroplasty for osteoporotic spinal fractures: surgery to fill a backbone (vertebrae) with cement
Arthroscopic debridement for osteoarthritis of the knee: inserting a tube to remove tissue
Laparoscopic uterine nerve ablation for chronic pelvic pain: surgery to destroy a ligament that contains nerve fibres
Removing healthy ovaries during a hysterectomy
Hyperbaric oxygen therapy (breathing pure oxygen in a pressurised room) for a range of conditions including osteomyelitis (inflammation of the bone), cancer, and non-diabetic wounds and ulcers.
Our analysis combines the two big clues about questionable care: variation and ineffective care. It looks at treatments that we know are ineffective and identifies hospitals that are furthest from normal clinical practices.
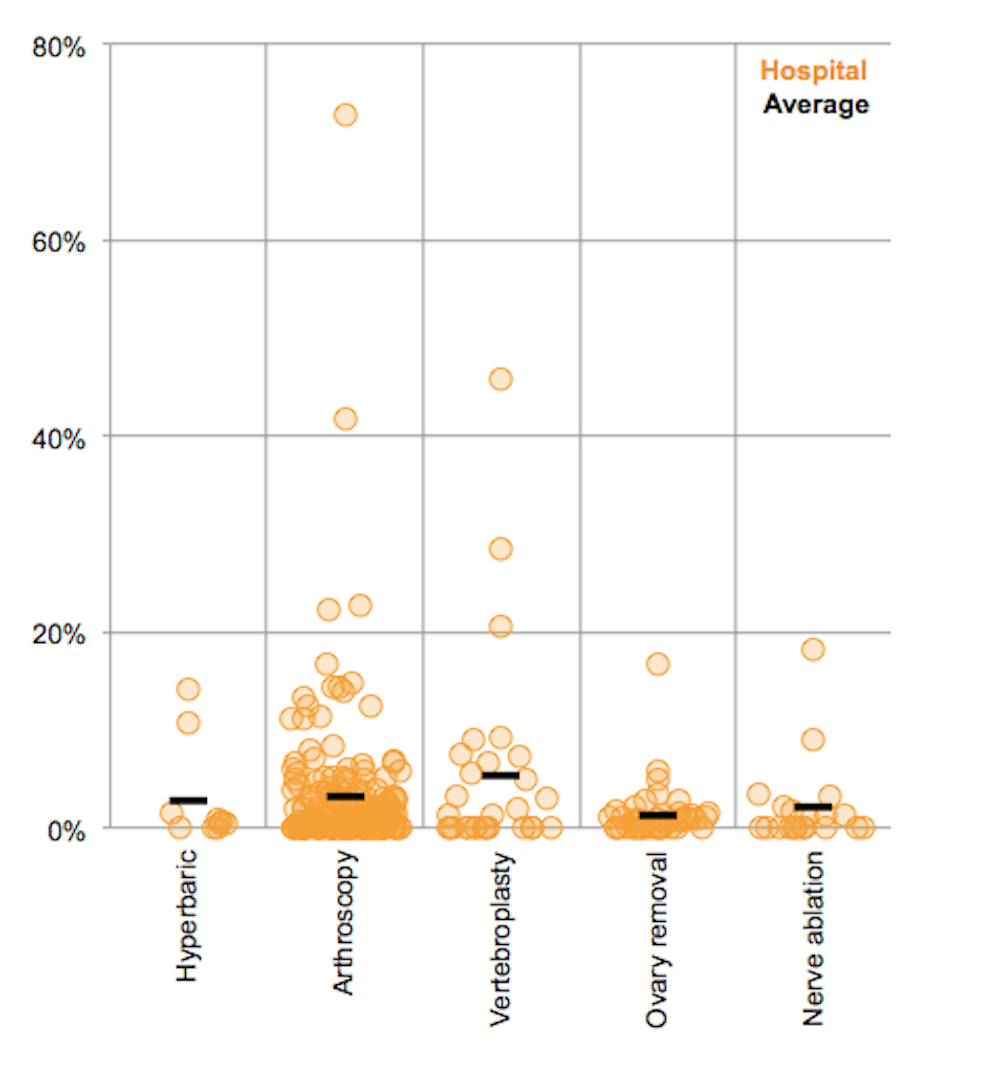
This exposes outliers with troubling patterns of care. While many hospitals never provide the do-not-do treatments, some outlier hospitals provide them at more than ten times the average rate.
Some public hospitals give do-not-do treatments far more often than average
The Australian Commission on Safety and Quality in Health Care should report these results to hospitals, states and health insurers. Clinicians should know when they are out of step with the evidence and their peers.
But that won’t always be enough. When high rates of do-not-do procedures persist, states and insurers must take action. In theory, these treatments should never happen, but in practice they might sometimes be needed. For this reason, we recommend a cautious approach that uses data to drive expert clinical evaluation.
Public and private hospitals should be given time to examine their own practices. If after a year they still perform a do-not-do procedure at an above-average rate, the state government should initiate a clinical review of the hospital’s practices. Then doctors who perform the procedures can explain why to their peers.
The hospital’s practices may turn out to be justifiable. But if they aren’t, there should be consequences: states and insurers should start withholding funding for the do-not-do procedure.
Our report provides a proof-of-concept for this approach. Many more do-not-do treatments can be measured, including those that should be performed, but not routinely (our report looks at a further three examples in this category).
For years there have been concerns that patients are getting the wrong treatment. Our Questionable Care report shows how to stop it.