

Women smoking while pregnant has been an uncomfortable reality for decades. Whatever the reason – whether a lack of concern about the risk, belief it’s too hard to quit or even reports that a resultant smaller baby will make for an “easier” birth – the reality is that a small baby that was meant to be bigger is at risk of stillbirth, cot death, future heart disease and shortened life span.
Substance misuse has affected all strata of society for millennia. And for several decades, researchers have been studying the effects of recreational drug use in pregnancy. An annual survey of more than 65,000 women in the US found that one in 20 pregnant women said they had used illegal substances, while one in 10 of the general population did so. These relatively stable rates appear lower than those identified in smaller UK studies, but what is clear is that rates are highest among pregnant teenagers and lowest in the highest maternal age groups.
Cigarette smoking was the first to receive attention, and this was followed by alcohol in the 1980s and subsequently given to other drugs such as marijuana, opiates, cocaine and methamphetamine. But although we have a wealth of knowledge about the risks, illegal drugs – unlike cigarettes or alcohol – don’t come with a warning label that says “using this substance while pregnant may harm your baby.”
One recent study from University College London suggested that using recreational drugs while pregnant put babies at risk of brain abnormalities. The study found that babies born with brain defects were twice as likely to have a mother who used illegal drugs in pregnancy than babies with normal brains. Of the 517 women studies, one in six had used recreational drugs – predominantly cannabis and cocaine – around conception or during pregnancy, which was confirmed by testing hair samples.
Crossing the placenta

Different substances might do different things and carry varied risks, but virtually all commonly used recreational drugs cross the placenta, where they are exposed to a developing foetus. Studies assessing these risks have been limited by both willingness of women to agree to testing (for example through urine or hair samples) or reliability of self-reporting. However, both animal and human studies strongly suggest that recreational drug use in pregnancy leads to problems from those that are visibly apparent at birth, such as cleft lips, to those manifesting in behavioural problems which may have consequences throughout adulthood.
Drugs may harm a developing foetus via multiple mechanisms and can vary depending on the stage of pregnancy. Direct effects on organ development are possible with drug use in very early stages of pregnancy, but evidence of this link beyond cigarette smoking is very limited, making the recent study from UCL a particularly welcome contribution. In later stages of pregnancy, more subtle effects include impaired delivery of nutrients that affects foetal growth and altered signalling within its brain.
Nicotine in cigarette smoke has been linked to development of cleft lip and palate, while heavy alcohol puts the baby at risk of foetal alcohol syndrome which disrupts development, with early signs including drowsy newborns and later problems including attention deficit and disrupted schooling.
Many pregnancy problems attributed to recreational drug use are common to multiple drugs, with the obvious example being poor foetal growth. This occurs commonly with cigarette smoking, heavy alcohol use and cocaine use, which has also been linked to smaller head size at birth. The effects are particularly prominent with alcohol as the effects are seen throughout childhood. These effects are likely to arise from restricted blood flow from the placenta. This also puts an unborn baby at risk of placental separation, which often results in vaginal bleeding, preterm birth and/or stillbirth.
Babies born to opiate-dependent mothers often suffer the effects of withdrawal syndrome following birth. This may include an unsettled baby with feeding problems, diarrhoea and seizures. The seriousness can be such that many such babies require an infusion of opiates to stabilise them before gradually reducing the dose until weaned entirely, which may take several weeks.
A mothers’ illegal drug use may also indirectly expose unborn foetuses to additional dangers – poor nutrition, for example, or exposure to violent situations, avoidance of healthcare and an increased likelihood of mental health problems.
Behavioural problems
Behavioural consequences of maternal substance abuse – the best known result from foetal alcohol syndrome – arguably gives rise to the greatest social burden, but tend to receive less public attention.
The behavioural effects of cigarette smoking and opiates appear to extend into childhood, with impulsive behaviour and attention problems particularly problematic (one study on cocaine suggested environmental factors also play a key role). Tobacco and alcohol have also been linked to delinquent and criminal behaviour, in addition to substance misuse in later life. Maternal use of cannabis appears to cause attention problems and impulsive behaviour about the age of ten, while metamphetamine also leads to drowsy or stressed babies.
In parallel with behavioural problems are those affecting thought processes, with recreational drug use in pregnancy resulting in impaired ability to memorise, analyse and problem solve, with or without a lower level of intelligence as measured by IQ. These problems are particularly apparent with heavy alcohol use, while cannabis appears to cause difficulty with problem-solving skills that require sustained attention. Cigarette smoking may impair language development resulting in poor language and reading abilities in children aged nine to 12.
Happens to normal people

Many of the risks described above can be mitigated by reducing or stopping drug-use in pregnancy. However, identifying who needs help isn’t straightforward because it is often a hidden activity. These women are not always in the heroine addicted, petty crime-associated circles of popular imagination, but may be part of outwardly thriving families, where boredom, loneliness or domestic abuse may lead to hidden substance abuse.
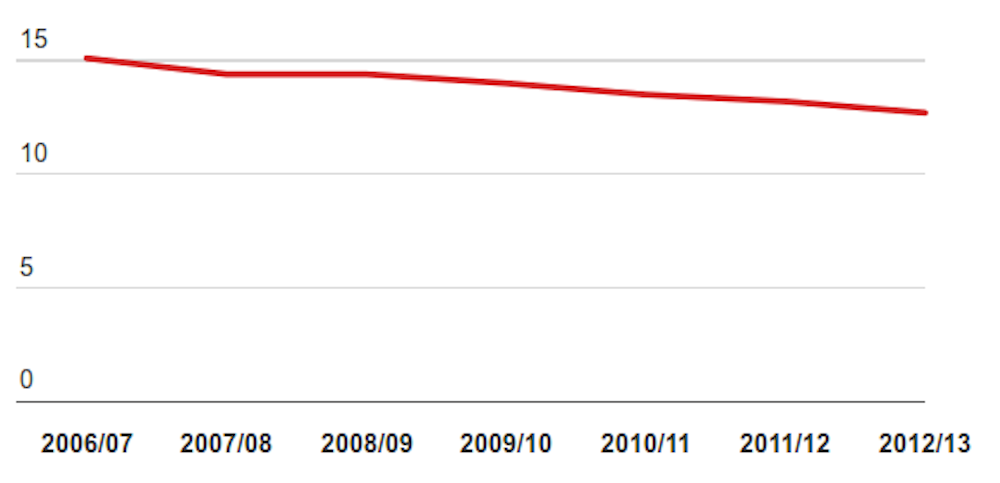
There has been a consistent fall in the number of pregnant women who class themselves as smokers in the UK (in England, the number of women who smoked in the 12 months before or during their pregnancy fell from around 15% in 2006-7 to 13% in 2011-12) and in the US.
This still leaves a significant number still but gives reason for optimism. But any possibility of this occurring in illegal drug use seems unlikely – these drugs aren’t used as publicly and so aren’t exposed to the same level of everyday scrutiny. These behaviours are also not subject to large-scale public health campaigns.
The mainstay of current treatment of recreational drug use in pregnancy is advice, support and detox, or replacement therapy. Alcohol detoxification is offered to those heavily dependent on alcohol, where risk of foetal alcohol syndrome is high. Opiate-replacement programmes, traditionally involving methadone, have enabled women to adopt more stable lifestyles and to regularly access healthcare.
This somewhat supportive and tolerant approach in the UK is in stark contrast to elements of policy in the US (though a recent UK test case of a mother accused of attempted manslaughter after heavily drinking while pregnant is currently in the courts). A rise in popularity of “crack” cocaine in the 1980s prompted some US states to legislate the reporting of any women known to use drugs in pregnancy for alleged child abuse or possible homicide.
The risk of this approach clearly include fewer women who are likely to come clean with their healthcare providers. Legislation was recently extended that obliges physicians to report all cases of newborn babies who show signs of drug addiction. But the impact of such legislature on actual drug-use in pregnancy or adverse consequences of the practice has yet to be seen.
The effects of using recreational drugs in pregnancy are wide-ranging. While many women who have used recreational drugs in pregnancy go on to deliver apparently healthy infants, severe problems may manifest in later years, whether encountering difficulties with education or displaying behavioural problems. Yet the enormity of the social burden on family dealing with such consequences may never be attributed to what happened during pregnancy.