

The Consumers Health Forum has just launched a website containing information about the cost of generic drugs in Australia compared to other countries. Each day, Australians pay A$3 million more for these drugs than they would if they bought them in New Zealand or the United Kingdom.
The information on the website shows the cumulative cost of current medicines pricing policy. Unless the policy is changed, that A$3 million will add up to A$1 billion in lost savings by this time next year.
How it works now
In Australia, the prices for most drugs are set by the government through the Pharmaceutical Benefits Scheme (PBS). The government pays some of the highest prices in the world for generic drugs (medicines on which the patent has expired).
Take the commonly prescribed cholesterol-lowering drug atorvastatin, for instance. For a typical dose (40mg), the wholesale cost of a script in Australia is A$38.
The comparative cost in England and New Zealand for the same drug is less than A$3. Based on last year’s usage alone, atorvastatin cost the Australian government A$548 million; if it had paid English prices, the drug would have cost A$119 million and with New Zealand prices, it would have cost A$100 million.
Atorvastatin’s patent expired around 18 months ago and wholesale prices have been falling since as many new suppliers enter the market.
But the price paid for atorvastatin by the Australian government has remained high because the pricing of all generic drugs on the PBS is governed by an agreement that’s due to end in July 2014.
Under this agreement, a mechanism known as price disclosure sets future prices based on past wholesale cost of medicines to pharmacists. The problem with price disclosure is the rate of adjusting generic drug prices is too slow.
It currently involves collecting wholesale price information from the pharmaceutical industry for a year and it then takes another six months to implement the price changes.
So any discounts on the wholesale price of common generic drugs such as atorvastatin that flow to pharmacies do not translate into price reductions for the government or consumers for a period of up to 18 months.
Under current policies, pharmacies get to keep all of these discounts and they quickly add up to very large amounts. For a drug such as atorvastatin, more than A$400 million will flow to 5,200 pharmacies from wholesale discounts from the time it came off patent to December 2013.
Moving towards a better model
England also uses a system of price disclosure, but the cycle over which cost reductions are made is only three months – six times faster than what happens in Australia.
The figure below shows the current prices for the top eight generics in terms of total government expenditure in Australia and what we would pay if costs were equivalent to those in England.
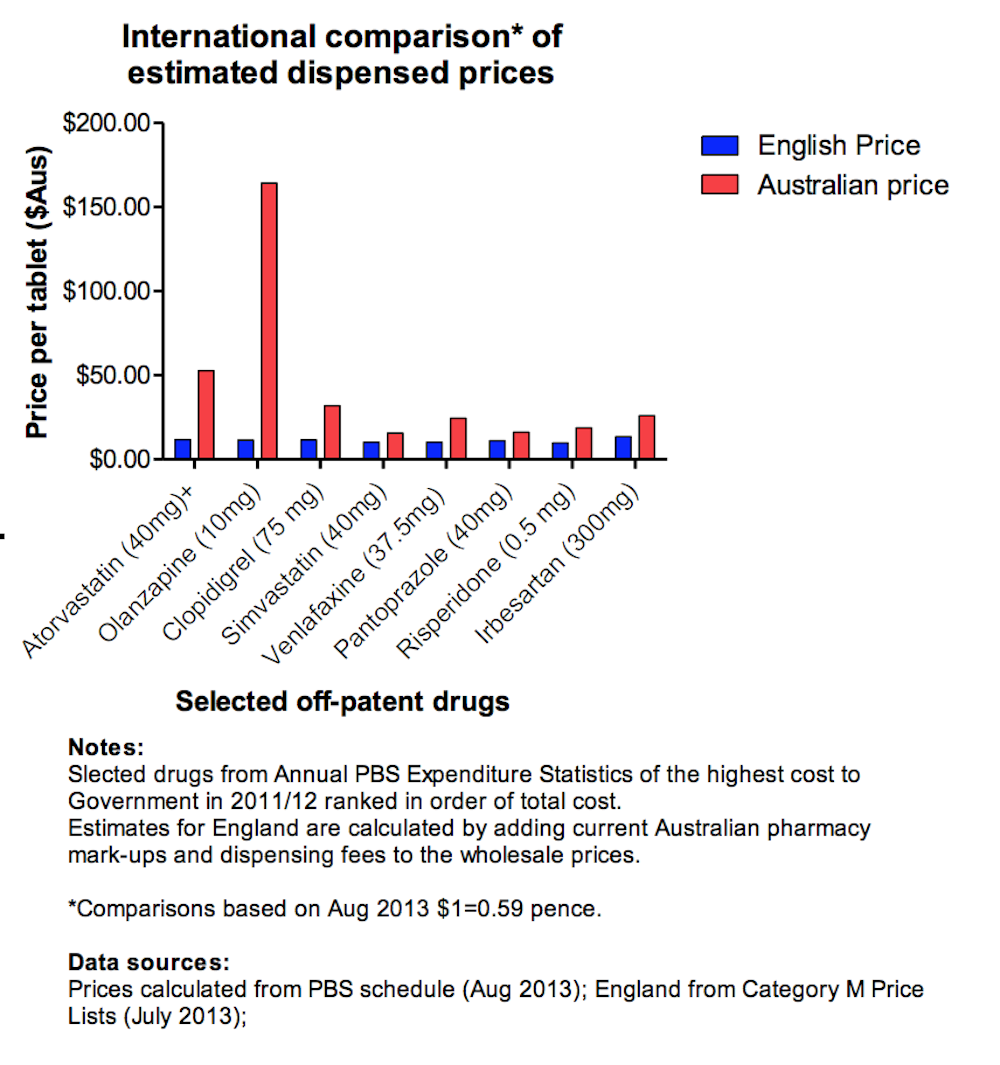
The speed of adjustment clearly makes a lot of difference.
For the 20 most expensive generic drugs, Australia pays around A$1.8 billion each year, whereas if the government could pay English prices, that would be reduced to around A$735 million, a savings of A$3 million a day.
How could we spend less? A first step would be to ensure that policy reform adopted by the previous government in its last economic statement is implemented.
Designed to take the first step towards speeding up the time it takes to adjust prices from 18 months to one year, the measure would return A$830 million from pharmacy owners to taxpayers or consumers.
In response to the changes, the Pharmacy Guild ran a political campaign arguing that up to 5,000 pharmacy jobs were under threat. And it indicated it wanted compensation for the changes.
It’s not clear if the new government will implement the reform and do more to reduce the prices of our most commonly used generic drugs.
Deja vu
Still, we have been here before. Tony Abbott introduced price disclosure in the final year of the former Howard government when he was health minister. He said at the time that it was a way to “harvest most of [the] discounts” that were accruing to pharmacy owners for taxpayers and consumers.
Abbott’s reforms included several hundred million in compensation for pharmacy owners for the loss of their discounts. But the payment was meant to be a one-off, as he indicated in 2006:
The reason why the savings to government become much more significant in five years’ time and beyond is because there are about 100 major drugs that are coming off patent in that time and we are compensating pharmacists, we are explicitly compensating pharmacists for the loss of discounts over the next four years; but we are not explicitly compensating them for the much greater impact of the loss of discounts in the subsequent five and more years.
The problem with the Abbott policy was that it was voluntary to supply real wholesale price data and industry chose not to do it for most drugs.
In the first round price disclosure reductions in 2009, the price of only four generic drugs fell. Commenting at the time, the Pharmacy Guild claimed that this debunked “myths about the extent to which community pharmacies are given discounts on generic drugs”.
Changes introduced by the former Labor government in 2010 were designed to fix these limitations, but their “accelerated” price disclosure was still an extremely slow process to reduce generic prices.
The most recent changes were simply a way of passing on these discounts more quickly to consumers and taxpayers. Isn’t it time all Australians shared in the discounts and got a slice of A$1 billion extra each year we are paying for common generic drugs?