


Any call for drug policy reform in the UK is usually met with a standard response from the Home Office. It goes something like this): “Drug misuse among adults and young people has fallen in the last ten years and we are working to educate young people about the risks, to help those who are dependent through treatment, and to clamp down on the illicit trade.”
Because drug use is falling, drug policy is working. Right? Well, not necessarily. As is frequently pointed out, prevalence is a poor indicator of policy success – harm is a much better indicator. A recent report by the Advisory Council on the Misuse of Drugs (ACMD) indicated that taking death as the most harmful outcome of drug use, UK drug policy is woefully inadequate – drug-related deaths have reached their highest level in over 15 years.
It is true that cannabis is rarely, if ever, associated with the most serious of drug harms, but that is not to say that its use is risk free. One indicator of harms associated with cannabis use is the increasing incidence of cannabis dependence and the rise in demand for drug treatment where cannabis is listed as the primary reason for needing treatment.
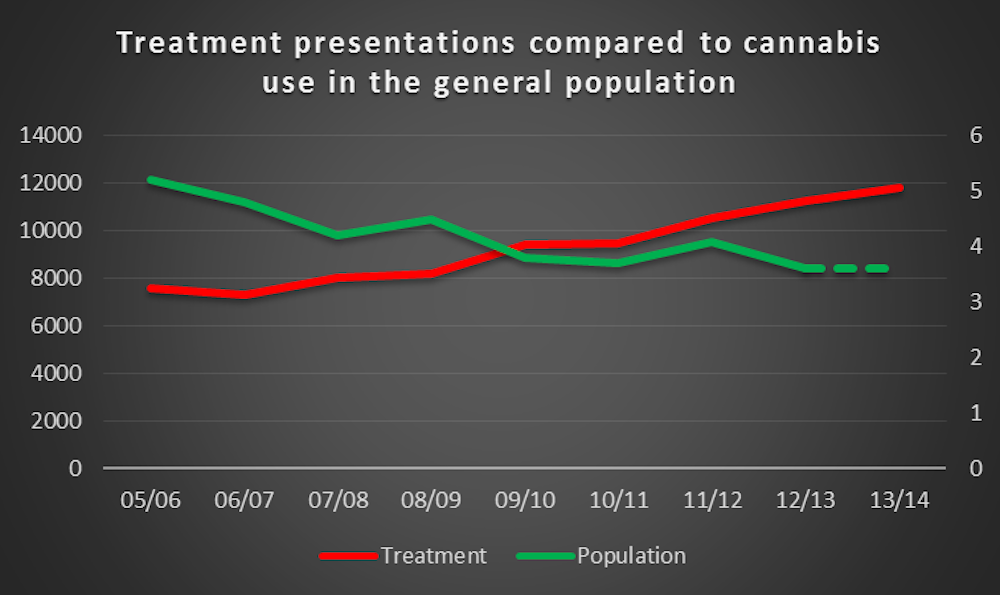
Treatment demand has been rising across Europe, but there is uncertainty over why demand for cannabis treatment is on the rise.
The policy campaign group VolteFace have published a timely investigation by Lizzie McCulloch into existing support for problem cannabis use. It highlights that it is unknown whether treatment is addressing a need that has always been there, with a “build it and they shall come” explanation commonly cited, or if we are seeing an emerging need in response to the prevalence of potent cannabis high in THC and low in CBD. Cannabis contains many cannabinoids, the best known is Δ9-tetrahydrocannabinol (THC) which gives you the buzz or high, while cannabidiol (CBD) is not psychoactive and is thought to counter the intensity of the high people experience.
Coercion
It also isn’t clear from the available data on referrals into treatment whether people are voluntarily seeking treatment or whether there is an increased level of coercion at play. Coercion is most often thought to stem from the criminal justice system, but it can take other forms, too. Softer forms of coercion might include a school or employer strongly encouraging an individual to seek treatment.
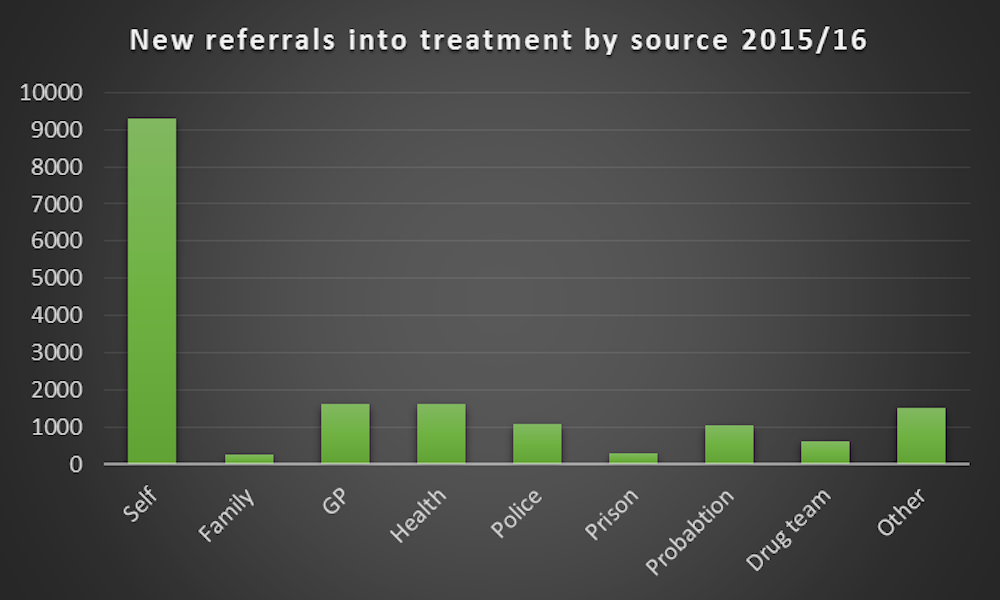
The publicly available data is of limited value. Referrals into treatment in the most recent Public Health England (PHE) data are not broken down by individual drug, but rather just by opiate and non-opiate referrals. For both categories, self-referral remains the most likely pull into treatment. However, there is a difference in criminal justice referrals, with non-opiate referrals – which will include cannabis – at 16% of all referrals compared to 10% for those with an opiate problem.
Similarly, a Freedom of Information request by VolteFace to Public Health England revealed how for over 18s, the majority of referrals came from the client, family and friends. The National Drug Treatment Monitoring System (NDTMS) data also reflects these findings, showing that non-opiate, and non-opiate and alcohol users are most likely to refer themselves, or through family and friends. They are also most likely to cite cannabis as a problematic substance.

Treatment
A combined referral source of self, family and friends does of course leave unanswered the question of whether significant numbers of clients are coerced by family or friends. Though it is possible that some individuals are being pressurised into treatment, the client group are adults who ultimately are free to make their own decisions. But even if a person were coerced into treatment, this does not mean that there is not a problem, nor that meaningful treatment cannot take place.
There are likely many reasons pushing people to seek treatment. One example is provided by a recent study which found a strong association between child abuse and developing cannabis dependency as an adult.
We should not forget that although we know enough about the frequency of drug use, we know little about its nature. Cannabis treatment presentations may be on the rise, but the consumption practices of regular, problematic users are still unknown in terms of the strains of cannabis consumed, whether cannabis is used solely or with other substances, and whether users or those around them perceive these activities as equally problematic. In short, understanding what motivates a person to seek treatment as a result of their cannabis use needs further investigation not least because it could have implications on treatment outcomes.