

Australia has a relatively strong health system by international standards, but it needs a makeover. To generate fresh ideas, The Conversation is profiling five international health systems that have important lessons – good and bad – to pull Australia out of its health reform black hole.
Much as many of us in Australia like to defend the status quo of Medicare and our health system, in reality, it’s best described as a dog’s breakfast. Policymaking, governance, funding and care are fragmented and complicated.
The Commonwealth funds and regulates pharmaceuticals, medical benefits, private insurance, and public hospitals – indirectly through unspecified grants to the states and now directly through activity-based funding.
State and territory governments fund and operate public hospitals and, varying by state, community care. Private insurers fund private hospitals and some medical specialist care.
All this has to be brought together by the user, especially if they have a chronic condition, and there they stand alone. A patient with diabetes, for example, needs ongoing care in the community from general practitioners and allied health and is more likely to require public and/or private hospital admission.
Each element of their overall care is the responsibility of a different funder. There is no single organisational entity with the knowledge, power and responsibility to support users achieve an efficient and effective outcome within the framework of a sustainable and equitable system.
Should we ever get the political will to significantly improve Medicare, we could learn some important lessons from the principles the Dutch government applied in its broad-ranging health reforms of 2006.
Health care in the Netherlands
Here’s how the new Dutch system works.
The benefit package: The government sets the benefits package of included services. These are essentially the same as Australia’s Medicare, covering general practice, medical specialists, pharmaceuticals and hospital care.
Setting the health budget ceiling: Each year the Dutch government sets an overall budget, based on predicted expenditure and revenue.
In Australia, there is no overall health budget ceiling because of the fragmentation of funding, with all elements uncapped, other than state funding of hospitals.

Raising the money: By law, 50% of the Dutch health budget is raised by a payroll tax (currently 7.5%) and a tax on other income (currently 5.4%), up to an income ceiling. This way overall health spending is tied to economic growth.
The government pays for children 18 and under, representing some 5% of the total.
The remaining 45% is raised by nominal premiums set by competing health funds and a compulsory annual deductible of up to €360. The average nominal premium in 2014 is estimated to be €1,120 per adult. This way everyone is directly involved in funding health care.
The nominal premium is regressive (that is, a larger proportion of a lower income person’s income than a person with a higher income) so the government provides an offsetting income-related “care allowance”, to a maximum of €864, via tax credits. Around 60% of the population receives some level of this allowance.
In Australia, Commonwealth health funding is derived from general revenue. In fact, the Medicare levy makes up just 18% of Commonwealth outlays on health. States also fund health from general revenue, much derived from Commonwealth grants.
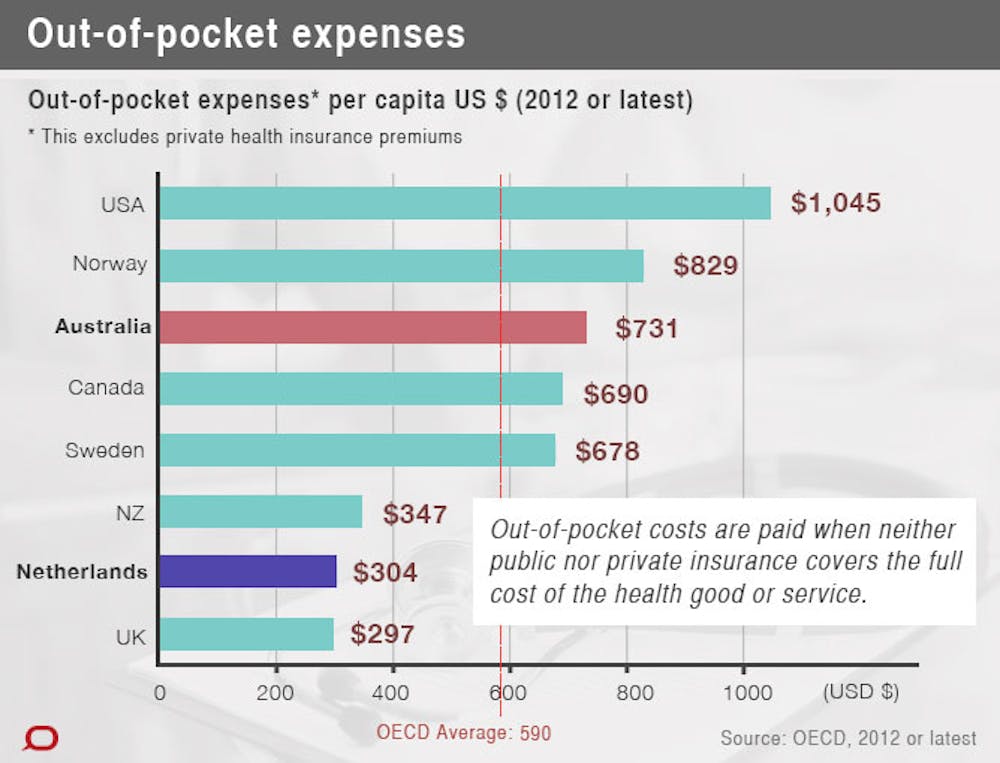
Australians contribute varying amounts to private health insurers and out-of-pocket payments, but the national average is A$731.
Competing funds: All Dutch citizens are required to have private health insurance with a fund of their choice. No one can be refused coverage based on their health, and premiums are the same for all members (for the same product).
The government provides independent web-based guidance for consumers, who are able to change funds each year, if they like. The funds are similar in structure and function as Australian private health insurers.
Funds also receive payments from the central pool of funding, based on the demographics of their members. This is determined by a sophisticated risk equalisation process that adjusts for predictable costs related to age, gender, chronic disease, recent high-cost care and socioeconomic factors such as region, socio-economic status and source of income.
Purchasing care: Dutch hospitals and specialists are paid per episode in a bundled payment, but unlike Australian activity-based funding that only funds hospital based care, this covers the period from referral by the GP to transfer back to the GP.
Around 70% of the bundled episodes of care in The Netherlands – mainly elective surgery – are subject to price negotiation between funds and hospitals. Through these price negotiations, funds can establish preferred “in-contract” providers.
The remaining high-cost, complex episodes of care have prices fixed by government.
GPs are paid on a mixed capitation, where they’re paid a lump sum to care for a patient over 12 months, and fee-for-service basis. Australian GPs are paid via Medicare’s fee-for-service model.
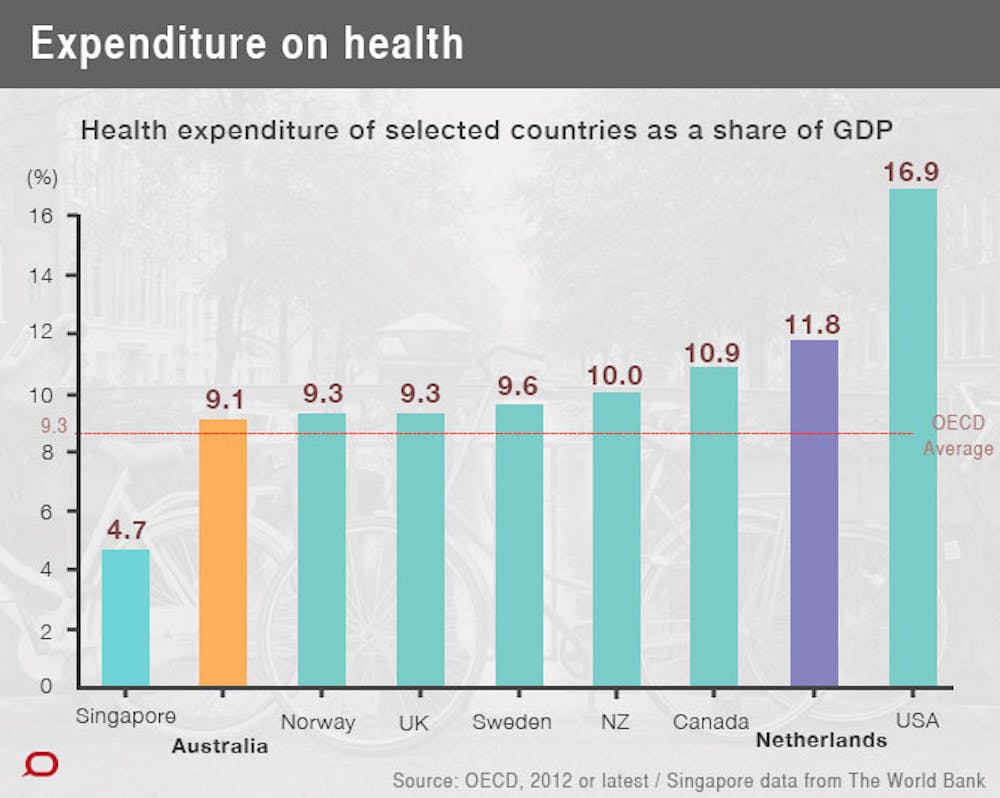
Performance: The Dutch health system is more costly than Australia’s. The Netherlands spends 11.8% of GDP on health, compared with 9.1% for Australia, and 9.3% for the OECD average.
From a consumer point of view, the escalation of costs has been minimal. The payroll tax has ranged from 7.2% in 2006 to a maximum 7.75% in 2011, after the GFC. And while the average nominal premium increased by a 8.7% in 2011, this came down to 2.2% the following year and -1% this year.
Competition between the main funds is active, but there is market concentration and regional niche players, similar to the Australian private health insurance industry. Members generally stick to one provider, however, with only a quarter having changed funds at least once since 2006.
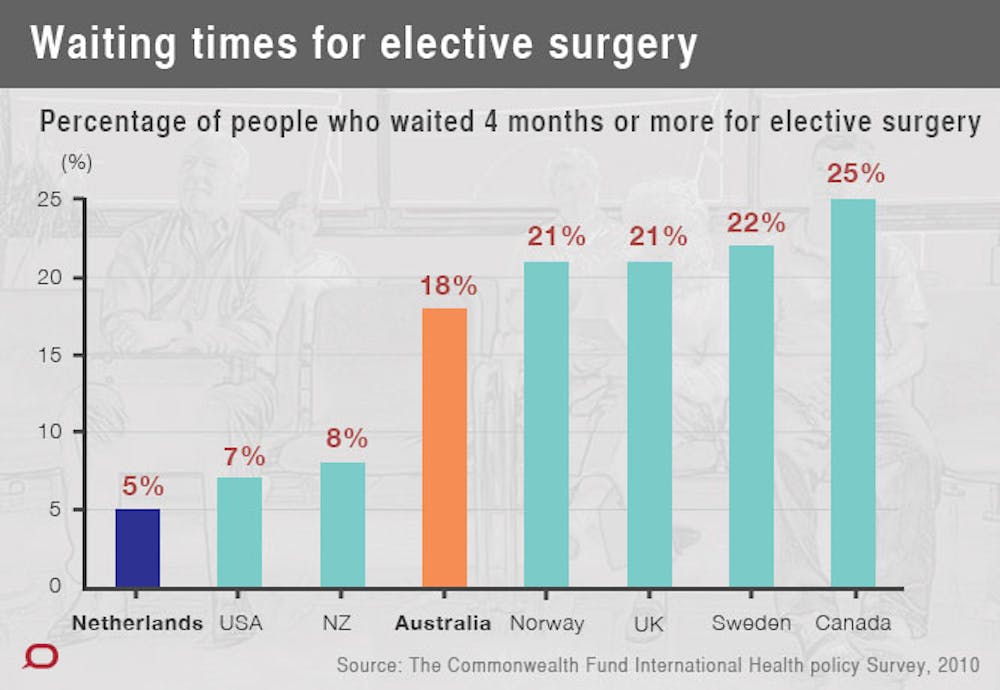
Importantly, the Dutch like their health scheme; the independent Euro Health Consumer Index consistently ranks the Netherlands as number one in Europe on patient-set criteria. Access has improved significantly since 2006, with waiting times for common surgical procedures dropping by up to three times – down to four to six weeks.
Long-term reform
The implementation of the 2006 Dutch health reforms has been cautious. It followed 20 years of debate and technical preparation.
The pace of competition has been managed, with initially only 10% of hospital procedures subject to price negotiations. This avoided large swings in provider revenue and enabled funds to develop purchasing experience.
Funds receive retrospective adjustments for unpredictable changes in membership and costs and, initially, between-fund adjustments to avoid large swings in fund profitability. This adjustment is being progressively withdrawn.

The system is truly universal in that it is the same for all. It is transparent, relatively simple and the engages the whole community in funding. Ask a Dutch self-employed taxi driver about the Dutch health system and they are likely to reply, as they have done to me on several occasions, “we have a terrific system, but it’s very expensive!”.
Australia has all the building blocks needed for a Dutch-style health system. Competing private health funds are gaining experience in provider purchasing and chronic disease management. And we have the appropriate regulatory process to oversee such a scheme.
Unfortunately, the politics of major health reform may be too hard for the Abbott government, as the Dutch health minister at the time bemoaned:
… when it comes to controlling costs the government always stands alone … while the established powers in the health care sector – and they are very strong ones – make every change difficult.
This article is part seven of The Conversation’s International Health Systems series. Click on the links below to read the other instalments.
- What can we learn from other countries’ health systems?
- Creating a better health system: lessons from England
- Creating a better health system: lessons from Singapore
- Creating a better health system: lessons from Norway and Sweden
- Creating a better health system: lessons from America
- Infographic: comparing international health systems
- Australian health care: where do we stand internationally?