



Australians have one the longest life expectancies in the world but are living with growing levels of lifestyle-induced chronic illness, according to the latest national health report card.
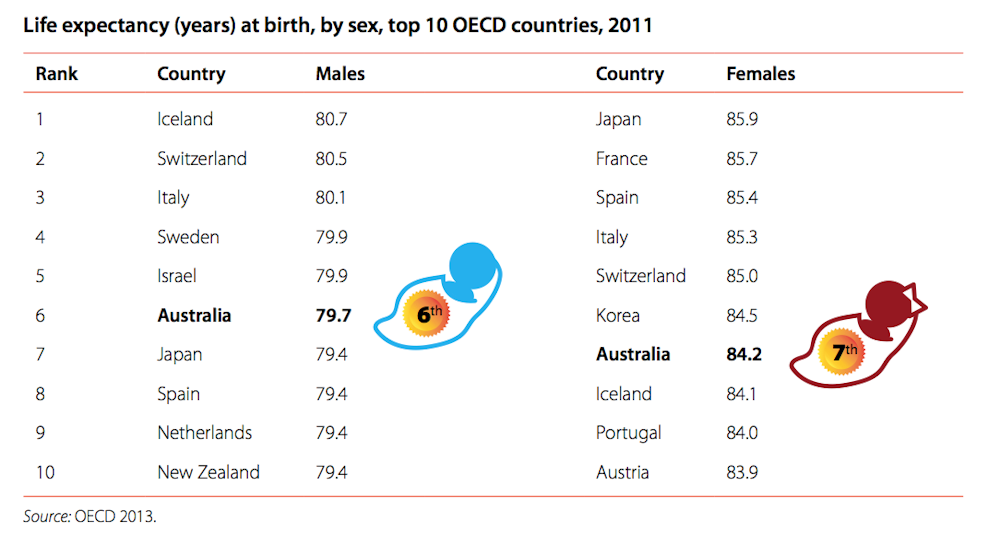
The Australian Institute of Health and Welfare’s Australia’s Health 2014, released today, shows Australians can expect to live about 25 years longer than a century ago – to 79.9 for men and 84.3 for women.
But life expectancy for Indigenous and rural Australians is much lower.
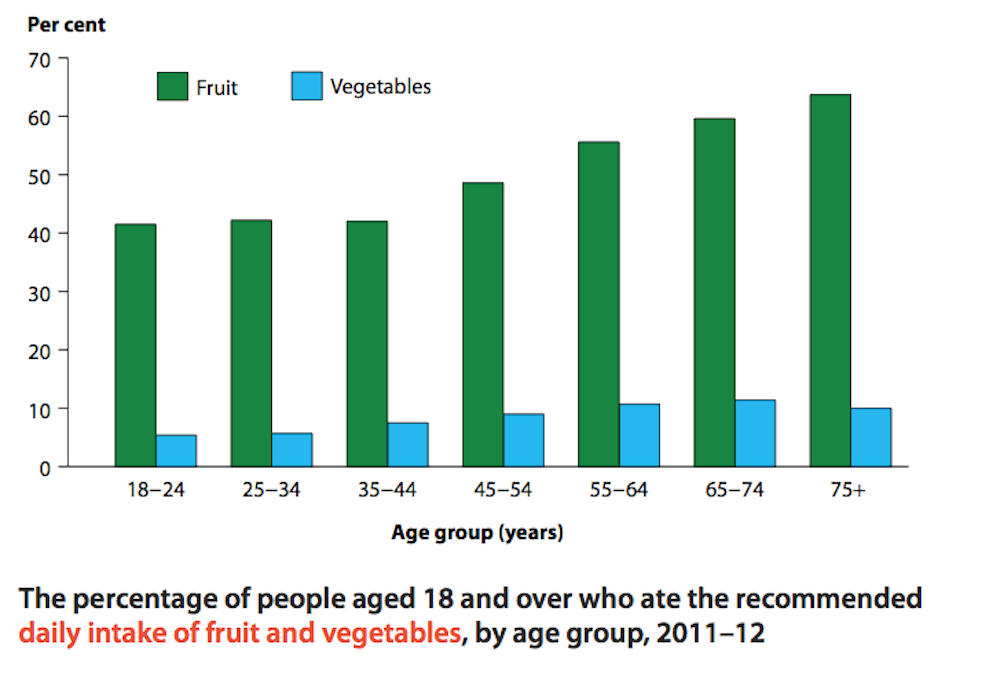
Excess weight remains a considerable burden on the health system, with 63% of Australians either overweight or obese. Around 43% of Australians meet the recommended minimum levels for exercise, with the just one in four over-75s sufficiently active.
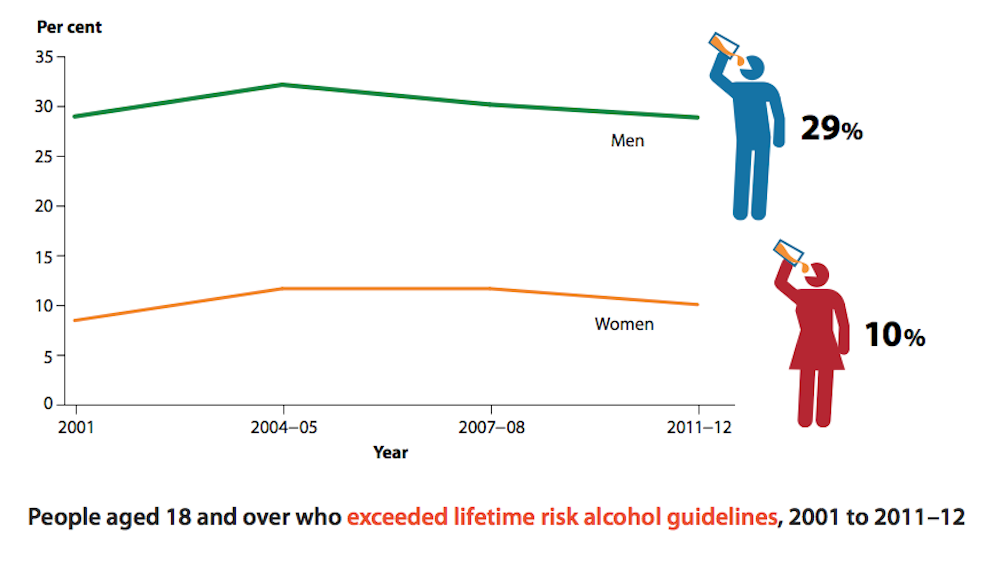
Almost one in five Australians (19.5%) consume more than the recommended maximum of two drinks per day, which has remained constant. But the proportion of people who never drink alcohol has increased slightly, from 10.1% in 2007 to 12.1% in 2010.
Chronic diseases are the leading cause of illness and death in Australia. Coronary heart disease remains the biggest killer, followed by:
- stroke
- dementia (including Alzheimer’s disease)
- cancer of the lung, breast, prostate and colon/rectum
- chronic obstructive pulmonary disease (principally emphysema and chronic bronchitis)
- diabetes.
On mental health, one in five Australians have had a mental health disorder in the past 12 months (3.2 million people). And 45% of adults will experience a mental health disorder sometime in their life.
The Conversation’s health experts analyse the report’s findings on lifestyle choices, health inequalities and the cost of care.
Lifestyle choices
Rob Moodie, Professor of Public Health at the University of Melbourne
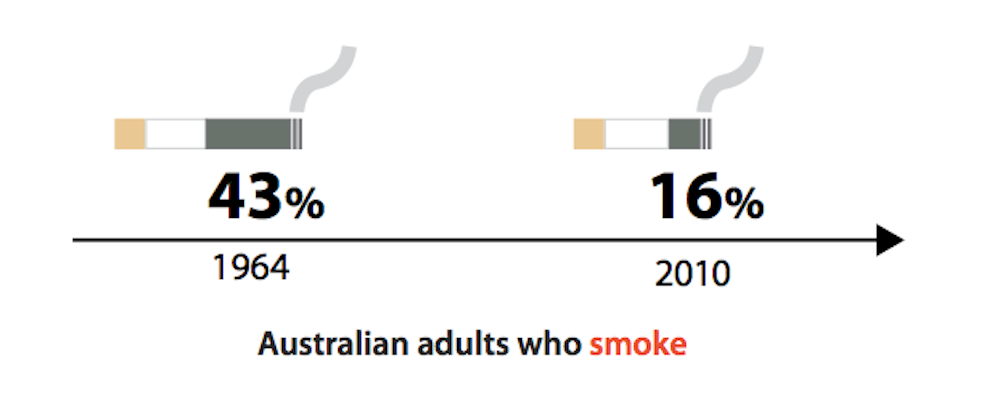
There is some very good news in this report. Life expectancy continues to rise, and years lived with disability decline. Smoking rates are dramatically down over the last 50 years (from 58% to 16%) and heart attack, cancer and asthma death rates are all falling.
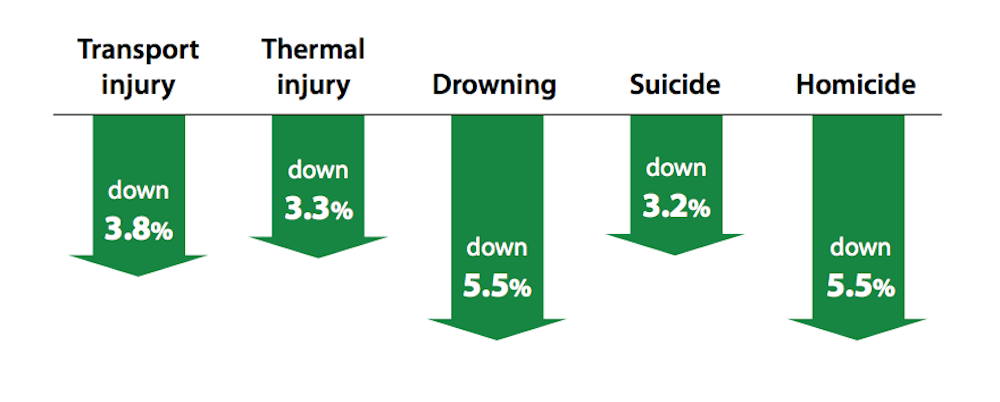
Injury deaths too, are down, and vaccination rates are improving – particularly at age five – and an increasing proportion of girls are being prevented from cervical cancer with the HPV vaccine.
The report shows our greatest health challenges are now chronic diseases, which are responsible for 90% of deaths in Australia. These are the non-communicable diseases (NCDs) including cancer, diabetes, cardiovascular and respiratory diseases.
We know that up to 80% of heart disease, stroke and diabetes and one third of cancers, the so-called “lifestyle” diseases, can be prevented by stopping smoking, shifting to healthy diets, increasing physical activity and stopping the harmful use of alcohol.
However, levels of excess weight and obesity in adults continue to rise and remain stubbornly at Everest-like heights for children. These are accompanied by very low levels (8% and 49% respectively) adhering to recommended vegetable and fruit intake, less than half exercising enough, and one on five Australians drinking more than two standard drinks per day.
Why aren’t we successful with managing our weight, our diets, our levels of exercise and alcohol consumption, as we have been with smoking, or skin cancer prevention? We do have choices, so taking personal and parental responsibility is part of the solution – and it’s a lot easier if you have high income, education and are employed.
But losing weight on your own, for example, is notoriously hard. As a nation we have put weight on together. I’m convinced that to lose it we’ll have to do it together, just as we have reduced smoking levels over time.
NCDs are not only “lifestyle” diseases, they are also “industrial” diseases fuelled by powerful transnational tobacco, junk food and drink, and alcohol corporations. The tobacco epidemic would simply not exist without the tobacco industry.
The biggest challenge we have is for the community to force changes in the behaviour of these unhealthy industries on the one hand, and for the best and the brightest in Australia to turn healthy food and physical activity into outstanding commercial successes on the other! If this happens then our personal and parental responsibility really can work.
Inequities
Sharon Friel, Professor of Health Equity, Regulatory Institutions Network and Director of the Menzies Centre for Health Policy, Australian National University
Unsurprisingly, Indigenous Australians, people from lower socioeconomic groups and rural dwellers continue to have poorer health and health outcomes compared to other social group. Averages mask inequities. So it’s good to see the summary report shine a spotlight on the stubborn, and in some cases worsening, health inequities in Australia.
One of the most egregious health inequities continues – it is incredible that an Indigenous boy born between 2010 and 2012 can expect to live more than ten years less than a non-Indigenous boy (69.1 years compared with 79.7 years) and an Indigenous girl about nine years less (73.7 compared with 83.1).
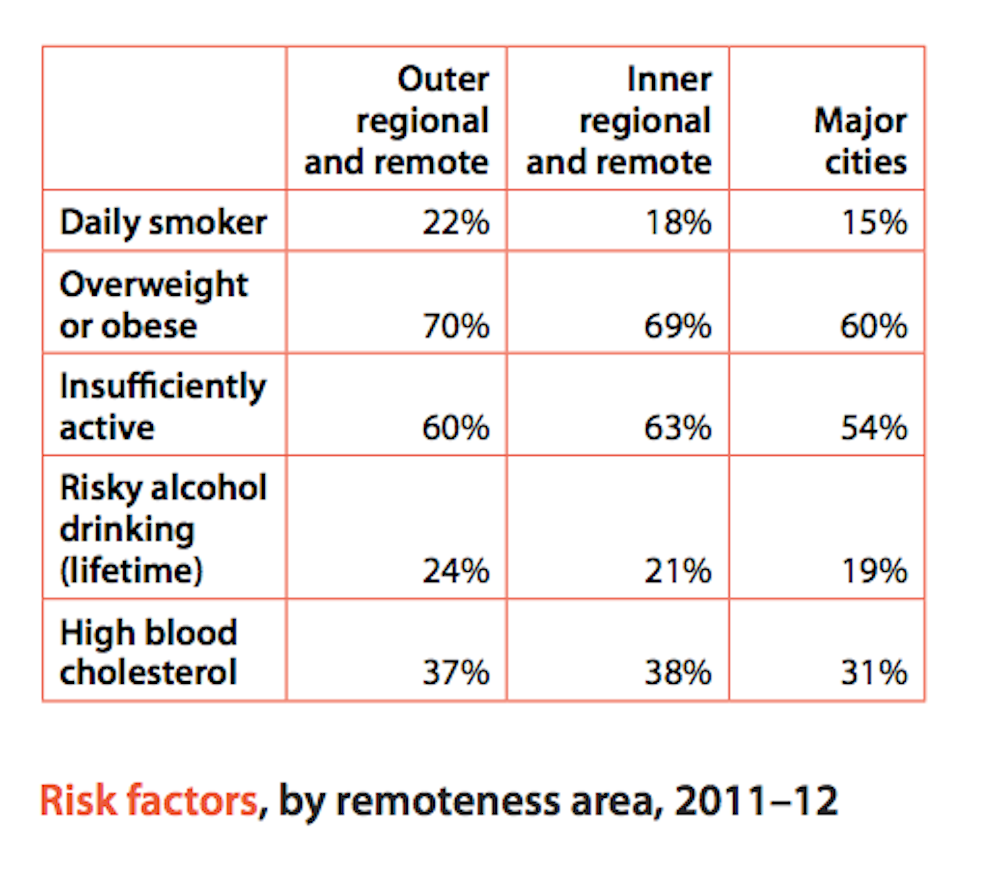
Inequities are also keenly observed between the health of people living in rural and remote areas compared to more urbanised areas. Rural and remote dwellers have less access to health services, travel greater distances to seek medical attention, and generally have higher rates of ill health and early death than people living in larger cities.
There is also a socioeconomic gradient in health in Australia. In 2006–2010, people living in lower socioeconomic areas had higher rates of early death from all cancers and lower five-year survival rates than people living in wealthier areas.
In 2011–12, the daily smoking rate was 23% in the lowest socioeconomic group and 10% in the highest.
People from lower socioeconomic status also experienced higher rates of lifetime harm from drinking alcohol (22%) than those in wealthier areas (17%).
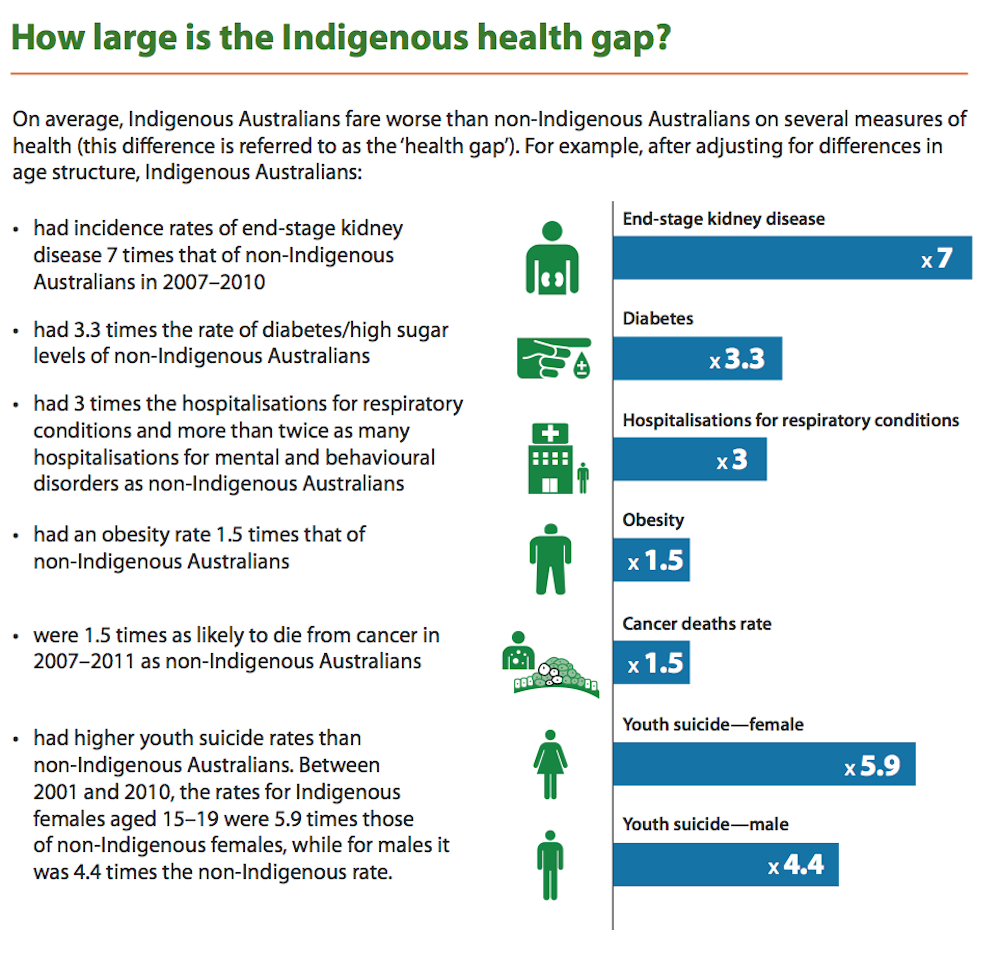
Why do these inequities exist and persist? The report provides a breakdown of the contribution of factors to the health inequities between Indigenous and non-Indigenous Australians:

If we want to address health inequities in Australia, we need to focus on the conditions in which people are born, grow, live work and age. We need policy and practice that aims to address educational disadvantage, lower employment and income rates.
And we need a real focus on removing the institutional racism that reinforces the health inequities between Indigenous and non-Indigenous Australians.
Rising costs
Professor Stephen Duckett, Director of the Health Program at Grattan Institute
The new AIHW report confirms both “known knowns” and “known unknowns”, as Donald Rumsfeld once distinguished.
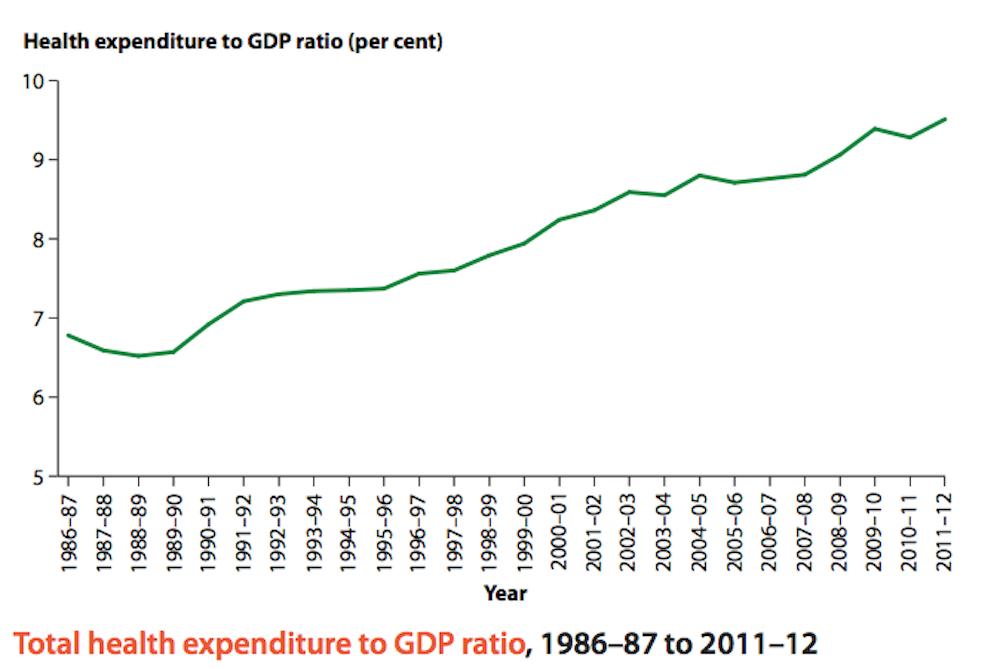
Health costs are rising as a percentage of GDP – over the last decade increasing at 5.4% per year compared to annual GDP growth of around 3.1%. But only Dickensian characters and the occasional politician focus entirely on costs, ignoring value or benefits for increased spending.
The report highlights that cost increases are significantly driven by new technologies – drugs and machines that lead to improved diagnoses and improved outcomes. Community expectations are also increasing, both in terms of expectations about the ability of technology to address health problems and access to those technologies.
The report, though, lists some important gaps in data collation:
there is a lack of information generally on the outcomes of health care in Australia, and limited information is collected on safety and quality, efficiency and cost-effectiveness.
The report also presents government health expenditure data in a new way, comparing the ratio of spending to receipts. After a decade of stability where government health spending was around a fifth of government revenues, the health share increased to more than one quarter.
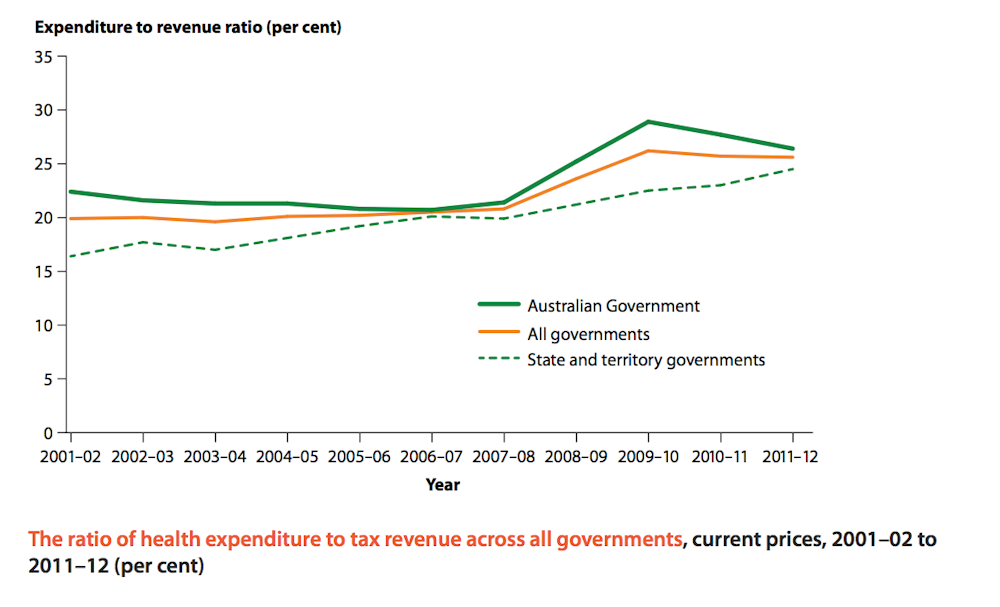
Importantly, the AIHW report highlights that this is a revenue side issue – the share increased because of a GFC-induced fall in revenues. With improved economic health, the ratio is now falling back towards a more comfortable position, at least for the Commonwealth.
The trend line for the states isn’t changing, showing a continued increase in the ratio of health spending to state revenues. This makes their squeals of pain following the 2014 commonwealth budget cuts to the states even more understandable.
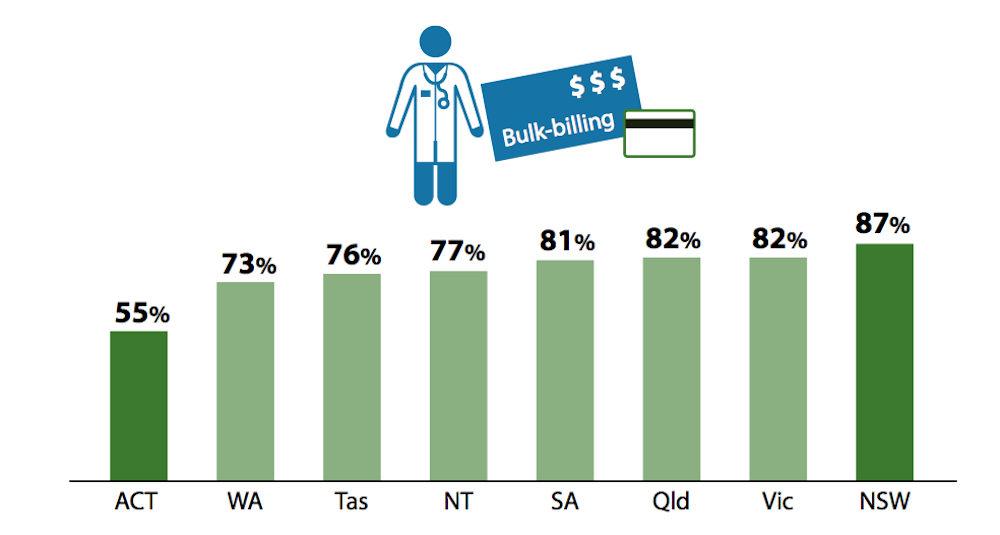
The report shows bulk billing is highly variable, residents of the ACT have to use a microscope to find a bulk-billing doctor (about 55% of services bulk billed) compared to much better access across the border in NSW (87%).
Finally, on access, the report presents a depressingly familiar picture: one in every 30 or so patents wait more than a year for elective procedures; one in ten wait more than eight months.