

Nations of the world came together in 2000 to make a solemn commitment to humanity to combat tuberculosis (TB), HIV/AIDS and other devastating diseases. This pushed governments to set up aggressive public health measures towards eradicating TB, but they have achieved only limited success. The moderate achievements have also been plagued by the paucity and poor quality of health data from lower-income countries.
But more importantly, while its Global TB programme marches on, the World Health Organisation (WHO) now recognises a critical unmet need. In 2012, the director of WHO’s Stop TB Department said:
Unfortunately, to a large extent, children have been left behind, and childhood TB remains a hidden epidemic in most countries. It is time to act and address it everywhere.
Don’t ignore children with TB
The full scope and extent of childhood TB is not known. This is because TB detection for that age group has often been neglected by those who collect health data, since children (defined as under the age of 15) were not considered to contribute to the spread of the disease or pose a high risk to others. Global plans to eradicate TB, drawn up by international bodies like WHO and the Stop TB Partnership, often omit any childhood TB-specific goals.
Diagnosing childhood TB is subject to many procedural and socio-economic challenges. The numbers, when reported, are muddied by deaths caused by other reasons, such as HIV, malnutrition, pneumonia or meningitis, resulting in severe underestimates.
The official 2010 TB data from WHO reported new disease cases segregated by age group, affecting 49,000 children all over the world. This considered only one measure of positive cases, and was likely an underestimate.
The 2012 Global TB Report represented the first concerted attempt by WHO to assess the childhood-TB burden, estimating 490,000 new TB cases and 64,000 deaths in children who had no HIV. The 2013 Global TB report puts these numbers at more than half a million new TB cases, and death of about 74,000 children.
A recent study published in the Lancet Global Health employed extensive mathematical modelling, and put together official 2011 TB and population data from WHO and other agencies, 2010 case notification data, with exposure predictions and natural history of paediatric TB. According to the study, 53m children were infected via exposure by 2010, with 7.5m in 2010 alone, of which 650,000 developed active TB disease, in the 22 high-burden countries.
This model yielded larger numbers compared to the WHO statistics. However, regardless of the calculation methods, these figures highlight the immense burden of TB disease borne by children across the world.
The scourge of TB
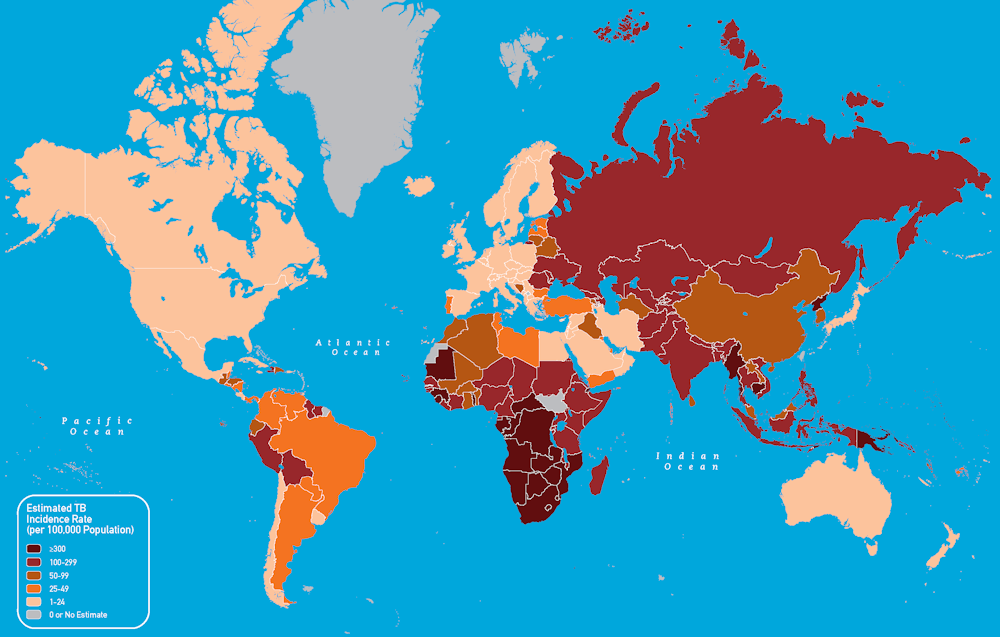
Of all the infectious diseases plaguing humans, the disease caused by rod-shaped Mycobacterium tuberculosis has contributed significantly to the global burden of disease throughout history. TB is contagious. When a diseased patient coughs, sneezes or speaks, the exhaled air carries microscopic, bug-laden droplets, which enter the lungs of others nearby. This exposure risk is especially high in regions of high TB prevalence, such as sub-Saharan Africa, parts of Asia, Central and South America.
Simply being exposed to the bug doesn’t cause disease. A series of immune defence cells can kill the bug. Only if one’s immune system is weakened – as in AIDS patients – or if the immunity is not robust enough – as in small children – the TB bug becomes active and starts multiplying inside the body. This is what makes TB the leading killer of people living with HIV/AIDS.
But because the TB bacteria has been around for a long time, it has learnt a few tricks of its own. These allow it to hide within the immune cells, and, when the environment is favourable, to escape the confinement and spread to neighbouring cells by subverting the immune cell functions. This means healthy individuals may become unsuspecting carriers of TB. This condition is called “latent TB”. It can become active TB years later, if one’s immunity is compromised.
How do doctors figure out if one has TB?
Doctors diagnose active TB by evaluating a combination of clinical symptoms via a skin or blood test, a chest X-ray and tests to find the presence of the TB bug. Recently it has become often necessary to test the bug for resistance to TB drugs.
Drug-resistant TB is an escalating public health challenge. The WHO currently recommends DNA-based tests for rapid diagnosis of such patients.
The diagnosis of latent TB is of great importance but it is challenging. The disease is unrecognisable in individuals who have no tell-tale symptoms. This leaves specialised blood tests as the only indicators.
These difficulties have made it hard to accurately estimate how many people have latent TB. Estimates could be as high as 2.3 billion, with one in every ten such individuals likely to have active TB during their lifetime.
Once diagnosed, TB is treated by using a combination of several anti-tubercular drugs, usually for six to nine months. To ensure all the bugs in the body are dead, it is essential to complete the entire course of all drugs. Treatment of latent TB requires fewer drugs, but for the same time span.
Not adequately considering the children while assessing the disease burden has so long enabled the “hidden epidemic”. This can, and must, be addressed.
In 2013, taking stock of the successes of its Global TB program, the World Health Organisation (WHO) has acknowledged that the target of 50% reduction in active TB disease worldwide may not be achievable by 2015, the time set by the 2000 UN Millennium Development Goals. When the international community sets up a new deadline, they should accord childhood TB a higher priority.