

The poorest fifth of people in England not only have a lower life expectancy than the wealthiest fifth, they are also more likely to spend more years in ill health than the better-off fifth. Because their health is worse, the less well-off also make more use of NHS services – especially emergency services. This little acknowledged fact is fuelling the A&E crisis in England.
But many emergency admissions to hospital could be prevented if people had better access to GPs, nurses, hospital specialists and other healthcare professionals, especially for chronic conditions such as dementia, diabetes, cardiovascular and respiratory diseases.
Not just the poor are affected
People in the most deprived fifth of neighbourhoods in England are nearly two-and-a-half times as likely to end up in A&E, for a preventable emergency, as the least deprived fifth. As the graph below shows, emergency admissions would be nearly halved if everyone had the same rate of A&E admissions as the least deprived. In other words, nearly half of emergency admissions are attributable to inequality.
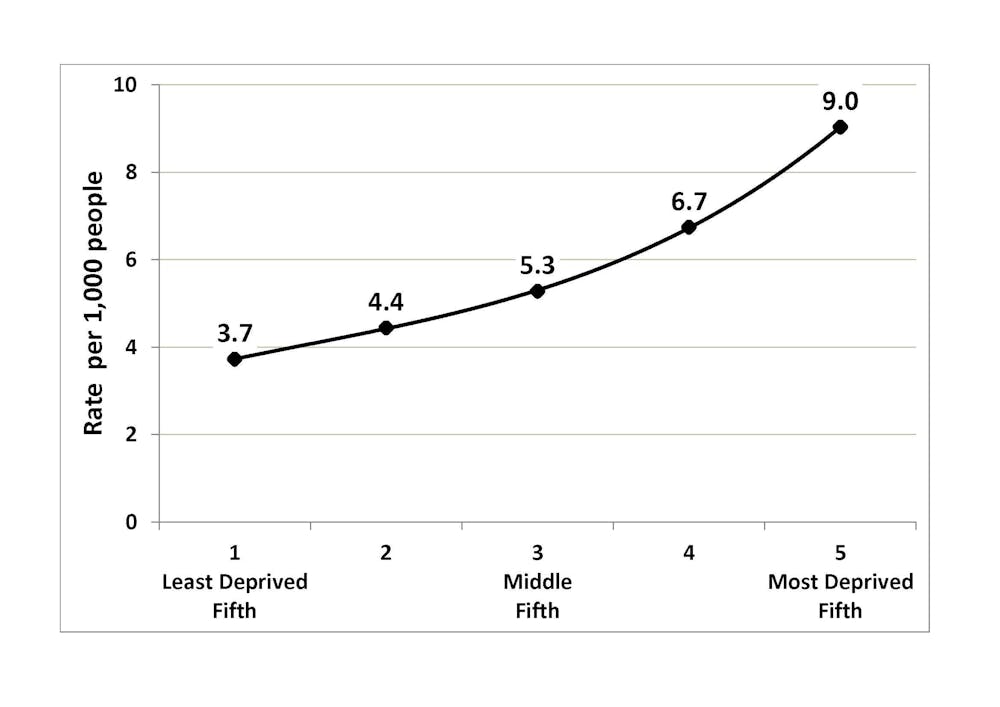
This problem affects everyone, not just the poorest. There is a “social gradient” in A&E admissions. The poorer you are – that is, the further down the gradient you are – the greater your chance of ending up in A&E.
Pressure on the NHS
In our recent research on NHS inequalities, my colleagues and I estimated that social inequality was associated with more than 158,000 preventable emergency hospitalisations in England in 2011-12 and nearly 38,000 deaths from treatable conditions.
Preventable emergencies are putting huge pressure on the NHS. This pressure is likely to become worse in the future as health and social care continue to absorb an ever larger share of public expenditure. The inexorable rise in costs is due to increasingly expensive treatments, people living longer with multiple illnesses, and rising wages in the NHS. Pressures from social inequality may also increase, if recent trends towards greater wealth inequality continue.
What can be done?
The NHS needs to develop new approaches to relieve these pressures if it’s to survive as a universal and comprehensive healthcare system. The NHS is good at providing equal access to GPs and hospitals when people suffer a health emergency. It’s not so good at providing care to people before they suffer an emergency.
NHS and local authorities need to become much better at this, by improving the co-ordination of patients’ care between specialties, between GPs and hospitals, and between health and social care. For example, patients at risk of repeated hospital admissions for breathing difficulties may need a follow-up to ensure they’re taking their medicines.
To co-ordinate care effectively, NHS managers will need better information about healthcare inequalities in their local area. Co-ordinated care sometimes requires paying closer attention to the less well-off, as advantaged people are often better able to care for themselves. They have better information, better support networks from family and friends, nicer home environments in which to recover from illness and sharper elbows.
Better information will help healthcare professionals identify who is at risk of preventable hospital admissions and follow them up. It will also help managers learn lessons from similar local areas that are doing well or badly at tackling preventable hospitalisations.
Barometer of social problems
Of course, the NHS can’t solve the problem on its own. A&E pressures are partly a barometer of wider social ills, and can’t be dramatically reduced unless Britain becomes more equal.
Wider action is needed by social services, education services and other public services that have an impact on people’s health. Action is also needed to change people’s behaviour, for example, through taxation, regulation and “nudges” to reduce consumption of tobacco, alcohol and sugar. Also, action is needed to reduce child poverty and improve early years education, as a poor start in life can lead to lifelong inequalities in health. The need for wider action on health inequality, however, should not be used as an excuse for NHS inaction on healthcare inequality.
Reducing healthcare inequality is a matter of social justice. And with A&E services being under such severe pressure from preventable emergencies, it’s also a matter of common sense.