
In 1984, artist Jon Cattapan’s sister Adriana died in a car accident. His painting, titled Sister, and some accompanying drawings, were a response to this tragedy. Sister depicts a grey-shrouded body lying on a bright red structure. Behind it are five figures in two separate groups. One represents living relatives and friends; the other, the spiritual world.
Sister’s distorted figures reflect Cattapan’s interest in primitivism and animism. Its colours and twisted forms project his anguish, and express the heightened intensity of the state of grieving. Cattapan has written about the disorientation experienced in grieving and also how the “topsy-turvy” space in all the Sister images represents his sister’s schizophrenia.
One day, a few months ago, a group of third year medical students spent a long time looking at these works, which were on display at the Ian Potter Museum of Art at Melbourne University.
They were encouraged by the Museum’s Academic Programs Curator to describe aspects of the painting as objectively as possible - its style, colours, content. Then they began to share their personal interpretations of the narrative.

Was the prone figure in the foreground dead or dying? What elements were more powerful? The Christian iconography and emotion on the figures’ faces? Their gestures? The insistent vibrancy of the colours? Or the apparently chaotic mix of formal elements? How did their interpretation change when the examination shifted to the Sister Drawings, hung alongside the painting, which are like snapshots of aspects of the story?
And how did the students’ initial gut reaction to the painting compare to the feeling it conveyed after 20 minutes of close, shared attention?
The aim was not to reach a consensus on what was going on in the artwork; rather it was to explore multiple alternative meanings. This was a practical demonstration of the medical method called differential diagnosis and the problems of rushing to a premature conclusion.
In response to the experience, one student wrote:
Objective things can have a number of different subjective meanings. People can have different perspectives. There is a lot of empathy required in order to extract these thoughts.
Teaching empathy
Healthcare professionals - doctors, dentists, physiotherapists, audiologists, optometrists - are now expected to have cultural, social and technical competencies that reach far beyond their biomedical training. And some clinical teachers have observed that graduates lack the capacity to demonstrate empathy or the skill of visually differentiating and prioritising what is important.
Can empathy be taught to these students? How can we ensure that they pay full attention to “the whole person” rather than just the disease?
Over the past two decades, there has been growing interest in the use of the humanities as a way of raising students’ awareness of emotions and the ethical dimensions of health care. Known as the “Medical Humanities”, many programs across the US and elsewhere engage students with theatre, literature, film and dance, as well as the creative arts.
The University of Melbourne began a pilot program at the gallery in June 2012 for six students in their Palliative Care rotation at Peter McCallum Hospital. It now provides programs to over 1000 students a year over 13 different areas in the health sciences, including Medicine, Dentistry, Optometry, Physiotherapy, Audiology, Nursing and Clinical Teaching. Unlike most such overseas programs, engagement is compulsory.

Medical students visit the gallery in First Year, and again in Third Year, when they are studying and doing hospital placements in areas such as Geriatric Medicine, Rehabilitation Medicine, Palliative Care and Psychiatry of Old Age. Over three hours, they work on attentiveness, interpretation, reflection and consideration of their emotional response.
Medical students particularly, and health students generally, tend to believe that there is a right and wrong answer to everything. This comes from their early training in pathology, anatomy and physiology, which is delivered under the bio-medical model, as compared to the bio-psycho-social model that the art museum sessions address.
Most healthcare students entering the gallery are already out of their comfort zones and in a state of alert curiosity. Their experience there, and particularly the diversity of perspectives that emerge in group conversations, demonstrates that you can have different interpretations of the same thing, without either of those positions being “wrong”.
Their teachers hope that students are beginning to realize that medicine is not black and white, but many shades of grey. The museum sessions are designed to get these students thinking about the importance of a diagnosis that is not just based on physical symptoms, but also on the larger narrative that informs a patient’s health story.
Moral imagination
Final year Physiotherapy students, for instance, were asked to draw upon their visit to the gallery to explore the question of ethics in healthcare provision, and develop what’s known as “moral imagination”.
The idea is for students to increase awareness of their emotional reactions to ethical issues, through looking at art, and enhance their capacity to recognise the moral dimensions of clinical experiences.
Students then write assignments based on their visit, incorporating both an analysis of ethical principals and reflection on their emerging professional identity.

After looking at the sculpture Twitch by Julia Robinson, which takes the form of a pair of soft, cream-coloured Long Johns with one apparently mis-shapen, exposed wooden leg, one student wrote:
There was no right or wrong way of deciphering the art piece and for once that was freeing. I left the museum somewhat changed…
Responding to a ceramic artwork by Stephen Bird – depicting a hand pointing to a bird on a branch accompanied by the inscription, “Singing not allowed!” – another student wrote:
The innocent looking bird, perched on a branch and trying to sing in its natural environment prompted me to think about a patient I saw lying in bed, calling out to medical staff, only to be dismissed as they are told that they are ‘doing fine’ or ‘need to continue with their course of treatment’.
This made me feel a little uncomfortable, as we are taught to practise with a patient-centred approach, listening to what others have to say and respecting their autonomy. What if the bird too, was singing out for help, only to be silenced?
Indigenous perspectives
Cultural understanding, particularly in the context of indigenous health, is vital for graduating doctors. Students are aware that they need this knowledge, but they sometimes consider the teaching to be guilt-laden. They have challenged us to provide more innovative ways to engage with this part of the curriculum.
One medical student, Mahesha Dombagolla, noted that
…a unanimously held sentiment by medical students is that we would find it valuable to gain some practical advice on how to provide care for Indigenous patients. Perhaps we can use Indigenous art to better understand their values and how we can incorporate these values when treating Indigenous patients?
For example, what are the Aboriginal perspectives on death/palliative care, caring for the elderly, women’s health, mental health, community and family, what things are respectful or disrespectful…?
In our programs, we now explicitly address Indigenous health, drawing upon Indigenous art to prompt discussions around cultural understanding and cultural determinants of health.

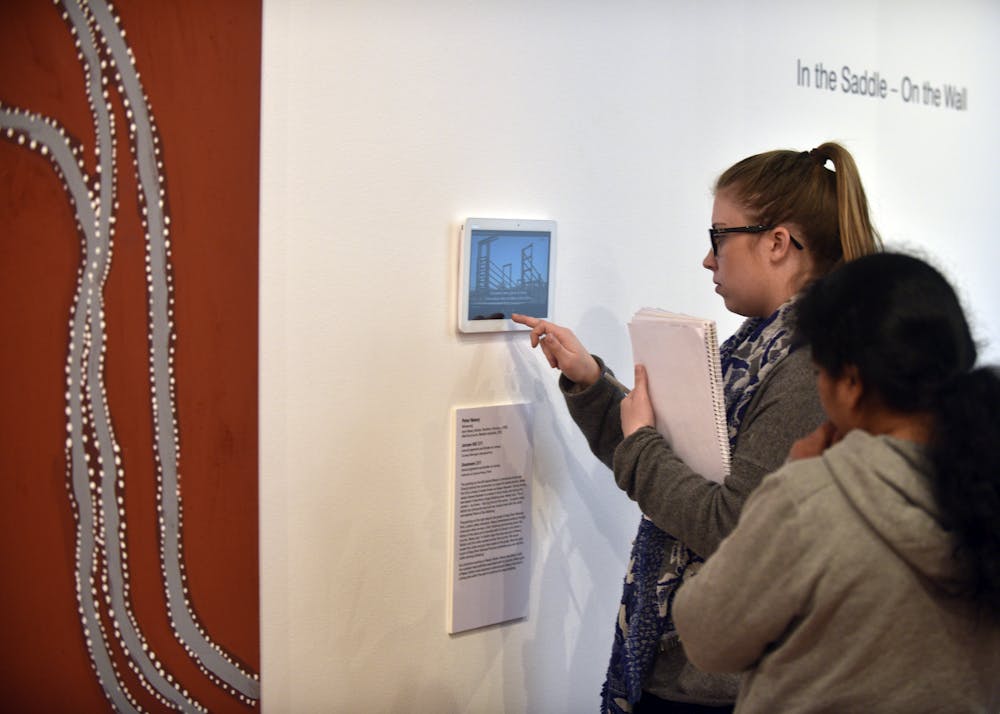
In recent months, we were able to engage students with the touring exhibition In the Saddle - On the Wall, which included both visual art and digital stories of Indigenous Elders from the Kimberley.
What students might assume as homogeneous experience of Aboriginality, and a “sameness” in life stories, was turned on its head as they explored the diverse life experiences of the 13 artists in the exhibition, and the different ways they expressed their life narratives and culture through paintings and interviews.
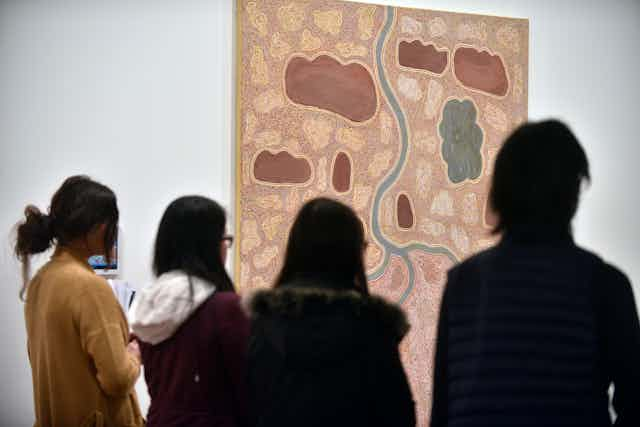
Our sessions focused on “other ways of seeing”, and the power of place in health and wellbeing. One painting the students examined, My Life My Family by Gija artist Shirley Purdie, gave a rich context for these conversations. A large square artwork created with natural ochre and pigment, it depicts aspects of the life of the painter, her parents and grandparents.
The visual narrative moves from the top right in a clockwise direction. A series of vignettes trace the violent events that caused Purdie’s family to move from Violet Valley Station to Mabel Downs station in the Kimberley, where they eventually settled and created a more peaceful life.
The work is testament to the agency and survival of Purdie’s family in a brutal, colonial world. The power of this story can only be unpacked by students through long and careful attention to both the artwork and the artist’s accompanying digital story. This is a great parallel to the care and attentiveness needed to provide professional, compassionate, and culturally appropriate care in Indigenous health contexts.
This narrative painting was in great contrast to many others that depicted Dreamtime stories and lore. Most students found these more abstract works harder to understand and interpret.
Looking at these paintings, students talked about the need to be patient, attentive, and to learn how and where to ask appropriate questions. While practising these skills with the artworks in group discussions, students considered their wider application in healthcare settings.
In contrast to the visual complexity of many of the artworks, the personal stories of the artists in the digital narratives were delivered in “matter of fact” style. This contrast prompted students to consider the different communication styles of people of different backgrounds - which will be relevant in their professional lives.

Students’ reflective essays give us great insights into the transformational experiences they had while viewing exhibition. One student said it “challenged my assumptions”. Another said the experience:
…enriched my knowledge about the hardship and troubles Indigenous Australians encountered. Whilst I was aware of the discrimination, abuse, and abduction, among other things that have occurred, it was still difficult to process these events, especially when hearing it from those who experienced it firsthand. I found it challenging to comprehend how the events happened and how these artists coped, as their lives are polar opposites to my own…
The combination of digital audio stories and paintings was especially powerful for the Audiology and Optometry students. One student observed that the way an artist spoke about his work was very different to the emotions expressed in his artwork.
… The artist I chose was discussing his childhood working on cattle stations and how it was a time of purpose and fulfilment for him. However, his body language in the video and the emotion in his artwork conveyed a more melancholy nostalgia. He talked in depth about how it gave him a purpose in life but skimmed over how he had to leave his family to do so. This example illustrates how in our profession we have to really listen (to verbal and non-verbal cues) to get the more personal information because people are not naturally comfortable opening up to strangers…
This exhibition also challenged students’ conceptions of ageing and agency by showing the influence the Elders exert both within their communities and beyond, in contexts that include health, welfare, and culture.
As one of the Mental Health Nursing students later tweeted,
Every painting is like every patient … they all harbour a story which we need to explore to better appreciate & understand them.
How effective is it?
While we know that museums can be agents of social change, there is as yet very little research around the pedagogical utility of art museums in intercultural understanding. Program evaluation is essential to convince academics and students alike that there are tangible as well as intangible benefits to their art museum visits.
At the Ian Potter Museum we have begun three ethics-approved research projects. The first is in Special Needs Dentistry, where we sought to develop students’ capacity to pay closer and more empathetic attention to patients, “beyond the tooth”.
Our research sought to identify any changes in empathy in the students, with tests done before and after the museum intervention. It found that the second year dental students had significantly high levels of empathy and generally perceived the art museum session as a worthwhile experience in terms of widening the scope of core clinical skills including observation and empathy.
Whilst the intervention itself did not alter empathy levels at a single time point, the findings did highlight the need for further investigation into dental student empathy over the course of their studies, and opportunities for increased targeted humanities interventions.
A qualitative survey of medical students’ experience of the program in the year following their gallery experience included interviews with museum and health practitioners about their perception of the educational value of these encounters.
Student responses in this study showed they valued the opportunity to learn observational, critical thinking and intra/interpersonal skills, but acknowledged difficulties in incorporating the humanities into the heavily scheduled and bio-medically-focused curriculum.
Another project in Medicine records students’ immediate responses after gallery sessions, followed by an online survey a few weeks later, exploring Indigenous health contexts as well as engagement more generally. Results from this study will be explored by a fourth year Medical student in 2017.
Clearly, for the majority of students, the experience is seen to be a valuable and memorable one. Fourth year Medical Student Kim Pham wrote that her sessions at The Ian Potter Museum of Art taught her about “taking the time to observe”. They also enabled critical discussion, which is essential to science but “often ignored during a packed medical curriculum”.
I left feeling more capable of engaging with the emotional narrative of my patients and being more open to their perspective.
Other universities around Australia are now creating their own programs for health students using their art collections. Flinders University, for instance, is teaching psychiatry students utilising works that include those in their rich collections of Indigenous art.
But in a crowded curriculum, sceptics might ask, is a visit to an art museum really a good use of students’ time?
We can’t yet prove conclusively that it is, but let’s end with more words from Kim Pham. Art, she says, has,
a capacity to make us critical and deep thinkers, using our capacity to observe to the full extent. And this should be a defining part of university education.
This article was written with the assistance of A/Prof Eleanor Flynn, A/Prof Clare Delany, A/Prof Mina Borromeo, Ms Bronwyn Tarrant, Dr Caitlin Barr and Ms Anthea Cochrane, Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne, all of whose students participated in engagements at The Ian Potter Museum of Art.