
The Movember campaign, which encourages men to grow moustaches each November to raise funds and awareness for men’s health, has helped raise the profile of prostate cancer. Statistics such as “one in eight Australian men will develop prostate cancer in their lifetime” provide men with an impetus to see their general practitioner (GP) and get tested for prostate cancer.
That’s good, right? Well, not quite. Not all men should be tested for prostate cancer. In fact, for some men, it can do more harm than good.
Testing for cancer
Testing for prostate cancer involves the use of two tests which can be done individually or in combination: the digital rectal examination (DRE) and the prostate specific antigen (PSA) test.
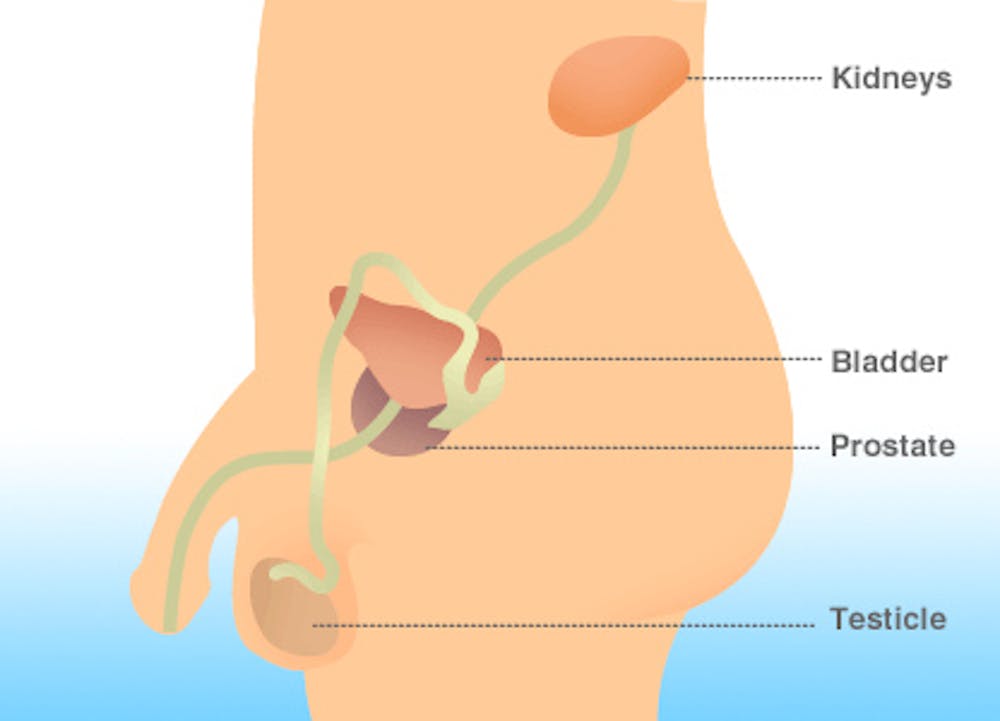
The DRE was commonly used as a front-line test for prostate cancer before the PSA test became available in the early 1990s. Use of the DRE in testing for prostate cancer is limited, since it is impossible to examine the entire prostate gland due to the anatomical location of the prostate gland itself.
Given the limitations of the DRE, the PSA test is commonly used as the front-line test for prostate cancer. PSA is a protein that is made in the prostate gland and can be measured via a blood test to assist in diagnosing prostate disease.
The PSA test is not cancer specific, as a raised PSA level may also be indicative of a benign growth of the prostate gland or an inflammation of the prostate gland.
How effective is the PSA?
A 2009 systematic review examining the accuracy of the PSA test in diagnosing prostate cancer determined the sensitivity of the PSA test ranged from 78% to 100%. This means the PSA test may fail to diagnose more than one in five cases where prostate cancer is present.
The review also found the specificity of PSA tests ranged from 6% to 66%, which means the PSA test may incorrectly “diagnose” prostate cancer in the majority of patients who test positive to the PSA test, when in fact, they do not have the disease.
This “over-diagnosis” is a common harm of PSA-testing, whereby patients who do not have any symptoms are diagnosed with a disease that would never otherwise cause them symptoms or lead to their early death.
Over-diagnosis may involve further investigation through an invasive biopsy of the prostate gland, followed by unnecessary treatment. This can lead to significant emotional and physical side effects including erectile dysfunction and incontinence.
The 2013 Cochrane systematic review on screening for prostate cancer, which pooled analyses of five randomised controlled trials, concluded that screening did not significantly decrease prostate cancer-related deaths but that harms such as over-diagnosis were common.
Conflicting advice
Professional organisations offer conflicting recommendations on the merits of and recommendations for PSA testing for prostate cancer, leaving middle-aged men understandably confused.
The Prostate Cancer Foundation of Australia (PCFA) recommends:
… men over age 50, or 40 with a family history of prostate cancer, should talk to their doctor about testing for prostate cancer using the PSA test and DRE as part of their annual health check-up.
The Royal Australian College of General Practitioners (RACGP) guidelines say:
Screening for prostate cancer is not recommended unless the man specifically asks for it; and he is fully counselled on the pros and cons.
Finally, the Urological Society of Australia and New Zealand (USANZ) argues:
… PSA based testing and subsequent treatment where appropriate, has been shown to reduce prostate cancer mortality in large randomised studies and therefore should be offered to men after informing them of the risks and benefits of such testing.
Much of the disagreement between medical and health bodies can be attributed to how evidence from the five randomised controlled trials is interpreted.
Only two of the trials, the European Randomized Study of Screening for Prostate Cancer (ERSPC) and the US Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial have been accepted as being methodological “sound”, yet provide conflicting results.
The ERSPC study reports a 21% reduction in the risk of prostate cancer death among a core subgroup of men aged 55 to 69 years, whereas the PLCO study reports no significant difference in prostate cancer death in men aged 55 to 74 years.
Differences in participants’ prior history of PSA testing, motivation to comply with the testing routine, PSA cut-off thresholds, screening intervals and treatment options, may contribute to the conflicting findings.
The ERSPC study, for example, used a PSA cut-off ranging from 2.5 to 4 nanograms per millilitre, while the PLCO study’s cut-off was 4 nanograms per millilitre. The PLCO study offered men annual PSA testing for six years and DRE for four years, while the majority of sites in the ERSPC study offered PSA testing to men every four years.
How professional bodies interpret these differences, and the weight attributed to each difference, may account for the disparity in recommendations.
So, should I get tested?
The RACGP provides Australian GPs with a clear recommendation not to provide PSA testing unless specifically asked. What GPs may struggle with is how best to counsel men about the benefits and limitations of PSA testing, given the usual ten to 15 minute consultation time. Decision aids and risk calculators, however, can help guide the discussion.
If you ask for a PSA test, your GP will likely ask why you’re concerned about prostate cancer and talk to you about your individual risk factors such as a family history of the disease. Your GP will also discuss the pros and cons of early detection and treatment.
On considering your absolute risk of developing prostate cancer and what benefit, if any, PSA testing may have, you’ll be better placed to decide whether it’s worth it.