


Welcome to our State of the Nation series, which looks at the coalition government’s progress over the past five years, across a range of key policy areas.
Coming in to the 2010 general election, most people thought that the NHS was in a good place. After significant under-investment over many years, the 2000s witnessed nearly a decade of sustained growth, extra staff, a significant focus on key clinical priorities (such as cancer, mental health and heart disease), greater emphasis on joint working with social care, a modernisation of buildings and infrastructure and – perhaps most impressive of all – a radical improvement in waiting times and access.
If someone had said in 1997 that waits would reduce from around two years in some instances to routinely under 18 weeks, most commentators (ourselves included) would have said it was impossible. And yet this is precisely what was delivered – public and patient satisfaction with the NHS was high and international comparisons were starting to look much more favourable. If ever there was a time for evolution rather than revolution, it was 2010.
With hindsight, this makes the massive (and arguably unnecessary) upheaval of then health secretary Andrew Lansley’s reforms even more tragic. Rather than building on what was working well and focusing on further improvement, the 2010 Liberating the NHS white paper threw this all up in the air, introducing an almost completely new system which still few people understand and most think can’t possibly work. The NHS is also undoubtedly feeling the strain of an ageing population, rising need and demand, significant financial challenge and a workforce that is overloaded and weary of change.
Unlike in 2010, healthcare will be a key electoral battleground this May – and all the signs are that this debate will be adversarial and bad-tempered. In thinking through how we got from the 2010 inheritance to now, here are ten things we didn’t know then but certainly know now.
Promises can be reneged on
What is said in opposition before the election and what happens in practice afterwards is often different: in the run up to 2010, the Conservatives promised there would be no top-down reorganisation of the NHS, before subsequently introducing the biggest top-down reorganisation in the history of the health service – one that NHS England’s former chief executive said was “so big you can see it from space”. (A similar story could be told about New Labour’s 1997 claim to end the internal market).
The story of this latest process is told in detail by Nick Timmins, but it is sobering to see how reforms which hadn’t been set out in a manifesto – and which few people anticipated or understood – could be introduced at such pace and scale.
Big structural change seldom delivers
Sometimes there are aspects that need to evolve or see radical change but (repeated) whole-scale reorganisation doesn’t work: structural “solutions” are often tempting as they look big and bold, and as if genuine transformation is happening. In practice, they reduce morale and productivity, distract attention away from improving patient care and seldom deliver stated intentions. It’s hard to exaggerate just how damaging such reorganisations can be – and the NHS Confederation has helpfully drawn attention to the constant “triumph of hope over experience” as we reorganise yet again.
Einstein wasn’t talking about the NHS when he described insanity as doing the same thing over and over again and somehow expecting different results – but this seems a good case study to back up his point.
Standing still isn’t enough
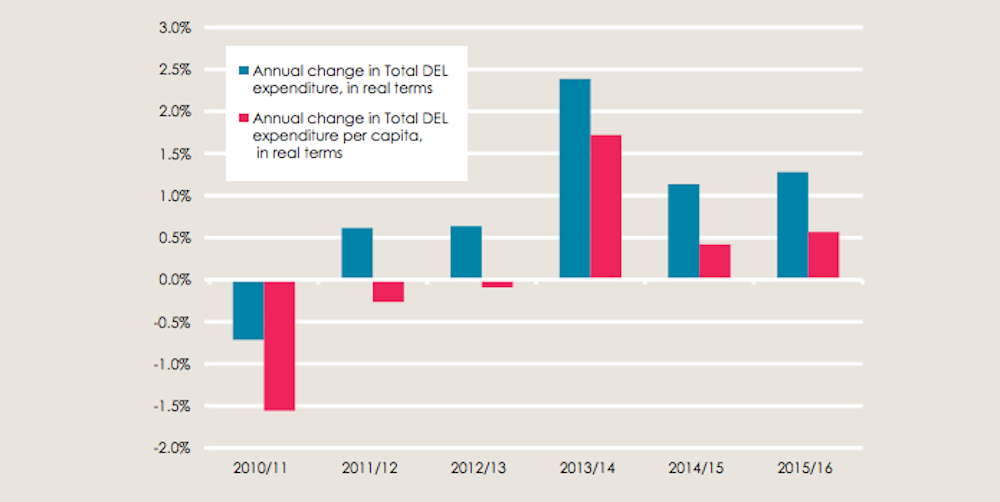
Ringfencing the NHS budget is still a cut in real terms if costs and demand are going up. Despite protecting the NHS from the cuts faced elsewhere, the health service still faces massive financial pressures (which in many ways spilled over during the A&E crisis).
Analysis by the Health Foundation suggests that spending has actually increased by an annual average of 0.9% – but that an increase of nearly 4% per year is roughly the figure which the NHS has needed over time – effectively just to stand still in terms of the ageing population and technological developments.
Listening to advice isn’t a bad thing
Sometimes people who point out potential pitfalls might actually be trying to help. From the very start, the Conservatives seem to have felt that the previous New Labour government lost vital time early on by being too timid in its first term – and therefore were desperate to be quick out of the blocks in a number of key policy areas.
With political leaders unused to being in government after such a long New Labour administration, there were inevitable mistakes and U-turns – and a tendency to assume that anyone offering advice about potential barriers and tensions was opposing reform. A greater commitment to listening – including to the concerns of the frontline staff and managers implementing reforms – rather than ploughing on regardless – might have yielded better results. A later “listening exercise” announced after mounting criticism came somewhat belatedly.
NHS ‘end is nigh’ is overstating it

No matter what pressures it faces, claims that this is “the end of the NHS as we know it” have so far proved wide of the mark. The NHS is so politically important that any debate about reform can quickly become polarised into a discussion about whether the changes amount to widespread “privatisation” (and about whether this undermines the founding principles of the health service). However, such terms are usually used in a very imprecise manner, with little clarity as to what “privatisation” actually means.
For example, the most significant private providers of NHS care are GPs, who aren’t public servants in a traditional sense and have historically operated as independent small businesses who sell their services to the health service. Despite this, GPs are routinely identified as one of the most trusted professions – and they are often seen as the foundation of the NHS. It is also apparent that the public still support NHS principles but are less concerned about who provides the care.
Local government has it worse
However tough things are in the NHS, it’s worse in local government which is facing what one leader described as “the end of local government as we know it”.

Local authorities have tried hard to protect adult social care spending – but directors of adult social services estimate that spending has fallen by 12% in real terms since 2010, at a time when the population of those needing social care support has increased by 14%. Councils have had to make savings of £3.53 billion on adult social care, with fewer people receiving support.
Actions speak louder than words
Care scandals can happen at any time – but talking tough doesn’t help. Events at Mid-Staffordshire, Winterbourne View and Morecombe Bay are truly shocking – and rightly led to much public soul-searching about how such terrible things could happen in a caring service. However, public inquiries with hundreds of individual recommendations, beefing up inspection regimes and ending careers only makes people more defensive and less likely to admit and learn from their mistakes.
By contrast, Yvonne Sawbridge’s work has demonstrated that an approach which pays proper attention to supporting frontline staff to deliver high-quality care is much more fruitful – and all the evidence suggests that happy, empowered staff achieve better outcomes for patients.
An answer with no question
Integration might be the answer – but we don’t know what the question is. Following the 2011 “pause” in Lansley’s health reforms, the work of the NHS Future Forum placed significant emphasis on the need for “integrated care” – joining up health and care services for older people and those with complex needs.
Over time, this became a key policy priority – but with very little clarity as to what it actually means or how to achieve it in a system not designed with integration in mind. While some sort of joint working probably has to be part of the solution, integration is no panacea and the system currently feels less integrated now than ten years ago. In response, many frontline services are starting to adopt a more healthily sceptical stance.
History shouldn’t define the future
The only thing we learn from history is that no one learns from history. Debates about integrated care are a good example of the loss of organisational memory which has been increasing with the churn of managers, new regulatory regimes and performance measures.
The current “integrated care pioneers” established by government to explore new ways of working, for example, seem very similar to New Labour’s integrated care organisation pilots (the results of which were underwhelming). Meanwhile the advent of clinical commissioning seems to overlook significant evidence around previous attempts at primary-care led commissioning. Finding new ways to balance the triple aim (improving access, reducing costs and increasing quality) will be more difficult if we don’t start learning lessons from the past.
Still delivering despite the struggle

Luckily for all of us the NHS still manages to deliver (almost irrespective of national policy). In spite of all the pressures, turmoil and upheaval, care quality is high, access does well and the NHS still has significant public support. Even during the recent pressures on A&E, most people continued to be seen in a timely manner – and it is testimony to the hard work and determination of staff that they kept the show on the road in very difficult circumstances.
Internationally, the Commonwealth Fund recently ranked the NHS first in terms of quality of care, efficiency and cost (with the US coming last), an improvement since 2010 when the UK came second.
The NHS is definitely struggling as we head into the 2015 general election – but also still doing well when we put current performance in context. With an outcome too close to call, any incoming government will have much to learn from the 2010-15 experience and much to ponder.