

The medical school at the University of St Andrews in Scotland is among those that still dissects human cadavers. Each year we allocate one body to between 12 and 15 undergraduates in first, second and third year, who work on different parts of it as an essential part of their anatomy studies.
The school – which has about 480 students in total – uses about 24 bodies each year, each of which is embalmed in the traditional way to preserve them for the duration. This makes them fairly stiff, with the advantage that it makes them easier for students to work with.
Anatomy then and now
The study of anatomy goes all the way back to such luminaries as Galen, da Vinci and Vesalius, spanning the first to the 16th centuries. Brothers William and John Hunter stand out in the 18th century as scientists researching anatomy as well as creating collections and museums that are still hugely admired and attended today.
The nature of anatomical research has completely changed since those days. When our knowledge of the basic mechanics of the human body was still developing, research enquiries were concerned with things like how the major organs worked, how they interacted, how they related to each other and to their blood supply and so forth. Nowadays anatomy is often used to describe research at the molecular level.
Researchers no longer dissect with surgical scalpels but by using high-resolution scans such as computerised tomography (CT) and magnetic resonance imaging (MRI). The dissection of cadavers is now mostly left to undergraduates and trainee surgeons.
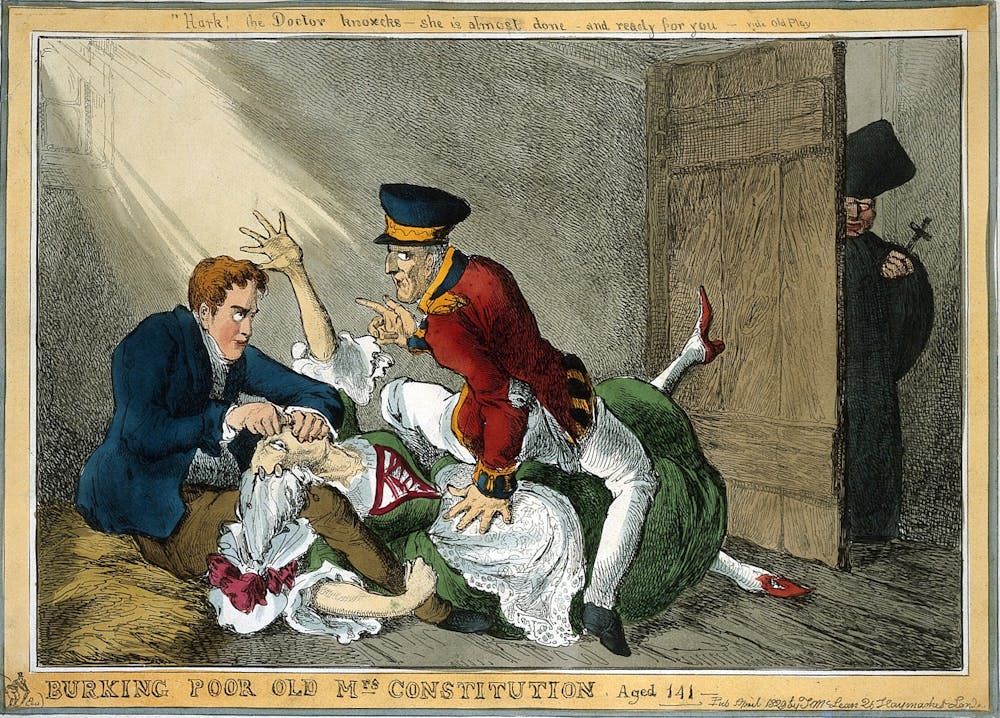
Back in the mid-18th century, only the bodies of executed murderers could be used for the purposes of dissection. As medical science became a higher priority in subsequent decades and the number of executions declined, the demand for bodies began to outstrip supply. This led to such atrocities as William Burke and William Hare committing multiple murders to supply bodies the Edinburgh Medical College in 1827/28. Fortunately these crimes triggered legislation in the form of the Anatomy Act of 1832, which introduced a licensing system that made medical scientists more accountable and broadened the kinds of bodies that could be used.
{kind=link}
Educational reforms
The system then remained stable for the next 160 years, until various events in the 1990s caused upheaval. On the one hand, the General Medical Council published a set of standards, Tomorrow’s Doctors, which sought to replace rote learning in medical schools with deeper understanding and vocational work from the early student years. In response, medical schools around the country introduced courses that concentrated on teaching basic science and clinical practice.

Anatomy was literally crowded out. Experiential learning by dissection was reduced, if not completely removed, and anatomy departments were subsumed into larger groupings. No doubt that decline was also heavily influenced by the fact that the old days of anatomical research were over and no longer attracted major grant funding or high-impact publications. Although anatomists like myself maintained research profiles, the discipline of topographical anatomy had become largely restricted to educating students.
By the mid-2000s we had reached a point where many medical students were graduating with a knowledge of anatomy that was adequate for general practice but not for anyone undertaking a career in an interventional field such as surgery, radiology or anaesthetics. Demand for cadavers for undergraduate study had decreased, which led to a misconception by the public and by doctors that it had fallen much further. Donations duly fell away, which brought us to the point where an anatomical resurrection became essential!
1990s body parts scandals
In parallel, the system for regulating human dissection hit a crisis as several scandals rocked the medical profession in 1998. Alder Hey Children’s Hospital in Liverpool and the Diana Princess of Wales Children’s Hospital in Birmingham were both found to have been harvesting the organs and tissues of babies who had died at their hospitals without anyone’s consent. Six months later, the two hospitals were back under the spotlight after it emerged that they had given children’s glands to a pharmaceutical company for research and had then received cash donations from the company.

{kind=link}
This prompted a review of the legislation, culminating in the Human Tissue Act of 2004 and the Human Tissue (Scotland) Act of 2006. This placed body donation under the regulatory supervision of the Human Tissue Authority in England and Wales and HM Inspector of Anatomy for Scotland, while finally making the whole process more open. The people who generously donated their bodies to science were assured of fully informed consent for the first time – and the choices within their bequests were made more clear and agreed in advance. Where previously giving verbal consent to a relative had been enough to become a donor, the reforms made the process much more official.
The reforms also introduced the option for donors to consent to surgical techniques and procedures, including the insertion of prostheses and implants. This led to an explosion in the number of surgical training courses based on the human cadaver. It also threw the path open for research into interventional techniques and methods of embalming that preserved the bodies more realistically – stiff embalmed bodies are not nearly as useful for practising surgery as they are for learning anatomy.
Surging cadaver demand
In the same way as the 1832 reforms, the system had been simultaneously tightened and liberalised. Medical schools, postgraduate deans and royal colleges for training surgeons now combined forces to create a continuum of anatomical education. Although teaching was augmented by a multimedia approach that included MRI and CT, computer-aided or virtual anatomy, anatomy apps, iPads and so forth, there was also a real increase in the use of appropriately preserved human cadavers.
This has particularly been at postgraduate level, but even undergraduate dissection has probably been restored to about one-third of what it would have been before the 1990s. Though nobody collates the numbers, there has been a huge increase in demand for body donation overall.
It would be easy to assume that computer-aided learning would become ever-more important in future, but there is no teaching substitute for putting a human cadaver in front of a group of medical students. It is hard to see undergraduate human dissection returning to its former levels, but neither is it likely to disappear again: the less you do at undergraduate level, the more becomes necessary at postgraduate.
Learning from the human body and therefore body donation remain essential. In following this route, we ensure that after death, we continue to inform life – and the living.