

George Osborne has announced that he would put an extra £2 billion into the NHS. This will be welcomed by many as an acknowledgement of the challenge faced by the health service in closing a significant financial gap in 2015-2016, which is likely to be one of the most difficult years ever for the NHS. Others, however, see it less favourably, as crisis management and an effort to plug a growing black hole.
And now there are reports that the £2 billion is not an entirely new injection of money, but that £750m of it has been diverted from existing funding within the Department of Health.
‘Real’ or not
The issue of whether extra money allocated to the NHS is “real” or not is not a new one. Endless debate has surrounded announcements by previous governments of all political persuasions about the degree to which extra spending on the NHS each year has represented real growth or whether it is already swallowed up by inflation and re-allocation to social care.
While there are still questions about what happened to the “extra millions” previously promised to the NHS, the health service has so far been protected from the radical cuts experienced by other departments as part of the government’s response to the economic crisis.
So does it really matter where the money for the NHS comes from as long as it is going towards supporting frontline services to improve the nation’s health? Well, yes, because the money could be used for other, valuable activities, which now have to be foregone.
In terms of the specific £2 billion dollar question, it seems that some of the money diverted from the Department of Health was the result of underspends – money from their budget that wasn’t spent. There are no details yet about what activities the money would otherwise have supported.
In an ideal world these will be things that would not have made as much of a contribution to improvements in health, as the diversion of cash to the frontline of the NHS will make. If that is indeed the case then we can quibble with the use of the £2 billion figure in the headline announcements, but not with the substance. But it is quite unlikely that such a comparison has taken place, in which case we don’t know whether the extra funds are better spent in this way, as opposed to the original intention.
Long-term prospects
From a broader and longer term perspective, extra money for the NHS cannot be found through successive underspends elsewhere in the health sector. So if money is being reappropriated to the front line, it may come at the expense of other departments’ budgets, with some consequences for the health and well-being of the population in other, less direct ways. These could include things like measures to reduce road traffic accidents or improve education, which also have an impact on citizens’ health and well-being. However, the fact that the public wish to protect the frontline NHS in preference to other public services is a message consistently reinforced through surveys and research.
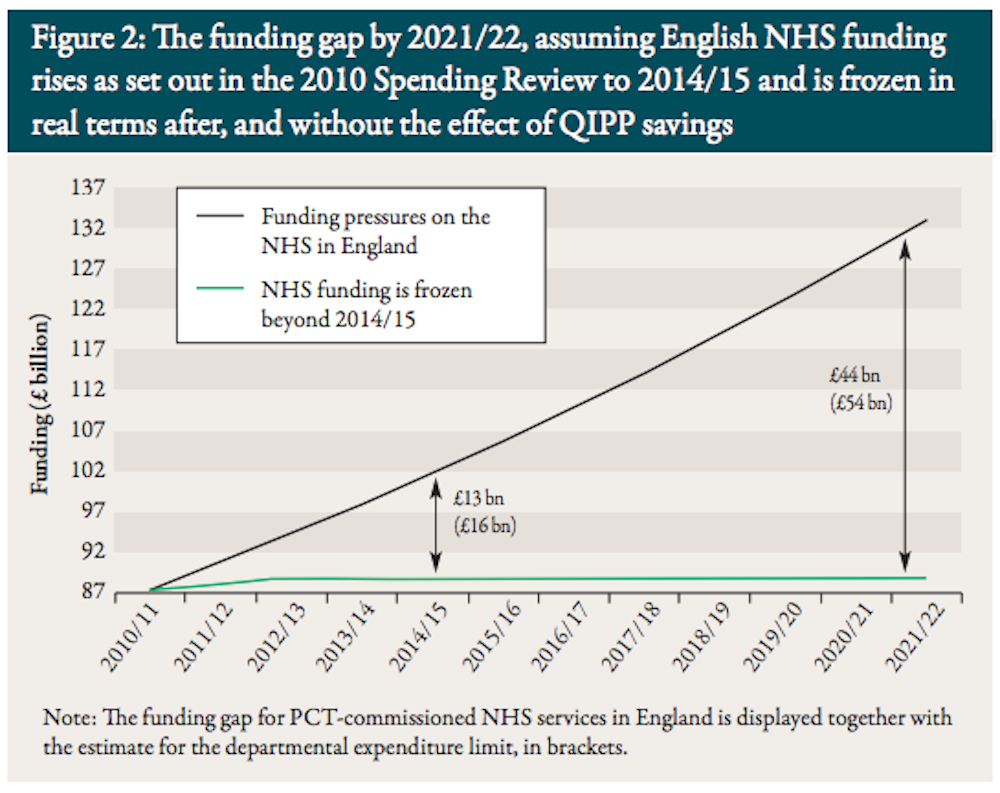
So what are the longer-term prospects for NHS spending? After all, the £2 billion, whether extra or not, is a drop in the ocean when compared to the annual spend of more than £100 billion. And, given the projected growth in the funding gap, well beyond £2 billion a year, finding extra money every year may prove impossible, even if ring-fenced. Hence the view that other more radical action is required, even if more money is found.
The most popular approach is to argue that the NHS has to make extraordinary efforts to extract more from every pound spent – the so-called “efficiency challenge”. This is feasible but some would argue it is not easy to do more with existing funds, without compromising on quality. Let’s remember that the NHS is faced with increases in demand and large numbers of hospitals are already running financial deficits.
This is part of the NHS Chief Executive Simon Steven’s argument, combined with plans for a more fundamental re-design of care provision and the financial mechanisms for health and social care. It is also hoped demand can be reduced through prevention and improving health promotion. Others will suggest that the time has come to bite the bullet and consider other means of supplementing the funding of the NHS from the patient pocket, such as charging for some services. But this is anathema to those who hold dear the founding principles of an NHS “free at the point of delivery”.
One thing is for sure: there is a lot more at stake than £2 billion and the debate will not stop here.