

Beep….beep……….beep……….beeeeeeeeeeeeeeeeeeeeeeeeep.
“We’re losing him. Out of my way, nurse!”
The quick-thinking young doctor charges the defibrillator paddles and places them on the chest of the lifeless patient, whose cardiac monitor is showing a straight green line. The patient gets a huge dose of electricity; his back arches and his limp body lifts up off the bed with the shock.
Seconds pass, then the familiar, comforting waveform appears on the monitor. The patient begins to stir, and is soon sitting up enjoying the healing properties of hospital sandwiches and a cup of tea.
You’ve probably seen this flatlining scene a million times on TV and films. Heck, they even named a Kevin Bacon film after it! It’s thrilling, compelling – and completely wrong.
To understand why this myth is so egregious, we need a quick background briefing on cardiac arrest.
The heart’s electrical system controls the organ’s ability to pump blood to the rest of the body. If the flow of this electricity becomes disorganised or the heart muscle stops responding normally, the regular pumping action is lost. Blood stops flowing and the body tissues have to cope with the sudden lack of oxygen supply. This is known as cardiac arrest.
We can see the various electrical wave patterns of the heart in cardiac arrest using an electrocardiogram or ECG. There are four main rhythms you might see during a cardiac arrest:
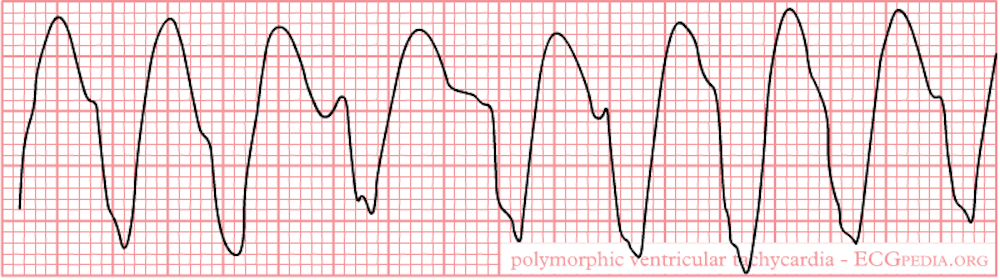
- Pulseless ventricular tachycardia (VT) is a very rapid and inefficient heart rhythm. The heart is beating so quickly that it can’t fill properly between beats. Circulation therefore drops rapidly to dangerously low levels.
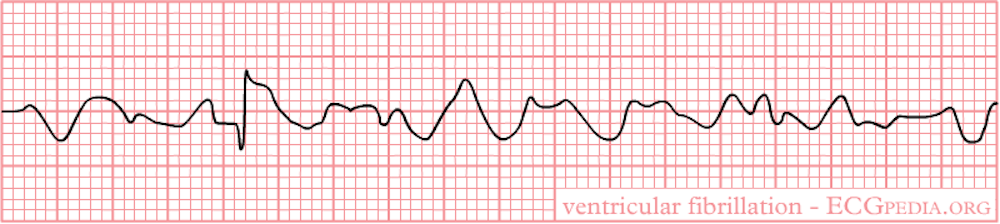
- Ventricular fibrillation (VF) is basically chaotic, unco-ordinated contractions of the heart muscle. Picture a heart quivering like a bowl of meaty jelly, unable to summon a proper contraction to send the blood on its way.
- Pulseless electrical activity (PEA) is where the heart rhythm appears normal on the ECG but the electrical activity is not producing any movement of the heart muscle. The lights are on, physiologically speaking, but nobody is home.

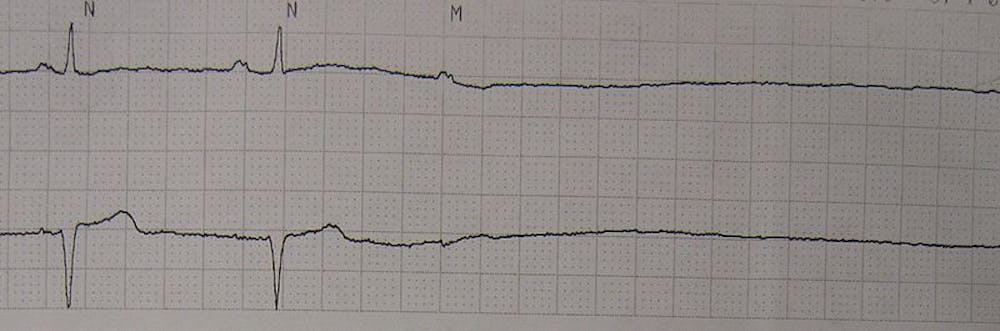
- Asystole (aka flatline) is the complete absence of any detectable electrical activity of the heart muscle. It appears as a flat line on the monitors. Clearly this is the worst type of cardiac arrest and there’s little chance of coming back from it.
These four ECG findings are classified into “shockable” and “non-shockable” rhythms, depending on whether they respond to the electrical current of the defibrillator.
Pulseless ventricular tachycardia and ventricular fibrillation (1 and 2) are shockable, largely because they tend to be caused by the electrical activity of the heart being thrown out of whack, and not by the heart muscle itself being badly damaged.
Hitting the heart muscle with a big dose of electrical energy acts a bit like hitting Ctrl-Alt-Delete on your computer (or Alt-Command-Esc for the Mac users). A single shock will cause nearly half of cases to revert to a more normal rhythm with restoration of circulation if given within a few minutes of onset.
Pulseless electrical activity and asystole or flatlining (3 and 4), in contrast, are non-shockable, so they don’t respond to defibrillation. These rhythms indicate that the heart muscle itself is dysfunctional; it has stopped listening to the orders to contract. The causes are hard to reverse and survival rates are very low.

The treatment of choice for asystole is to continue [CPR](http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Cardiopulmonary_resuscitation_(CPR) (cardiopulmonary resuscitation) and give a whacking great dose of adrenaline. In fact, if you stop CPR to give an inappropriate shock, the patient’s outlook is even more dire.
But unlike the famous overdose scene in Pulp Fiction might suggest, there seems to be no survival advantage and quite considerable extra risk of giving it directly into the heart. (I’m also ignoring the fact that adrenaline would be useless for a heroin overdose.)
So next time you see that ominous flat line appearing on the monitor, and hear the heroic physician shout “clear” while busting out the paddles, you can join the exasperated ranks of those in the know, and try not to let reality ruin this most dramatic of TV tropes for you.
This is the 100th medical myth and the last in the series. Click here to see the other myths we’ve busted over the past two years.