



The risk of death is high at birth and during the first years of life, but it decreases through childhood until approximately the age of 10. It then begins a steady, exponential increase that continues throughout adult life. This U-shaped curve of age-specific death rates suggests that the risk of dying for young adults should be relatively low.
Mortality can be high between ages 15 and 30
It is not rare, however, to observe relatively high levels of mortality during a period in early adulthood between the ages of 15 and 30. This is called “excess mortality” because it exceeds the levels that would be expected due to biological factors and epidemiological circumstances.
The relative scale of this excess mortality appears to be independent of the general level of mortality, as illustrated by the age-specific mortality curves based on data from the Human Mortality Database (Figure 1). They show situations for different periods between 1900 and 2018 in 45 countries with exhaustive vital statistics, mainly in Europe or other continents with populations of European origin, as well as a few Asian countries such as Japan.
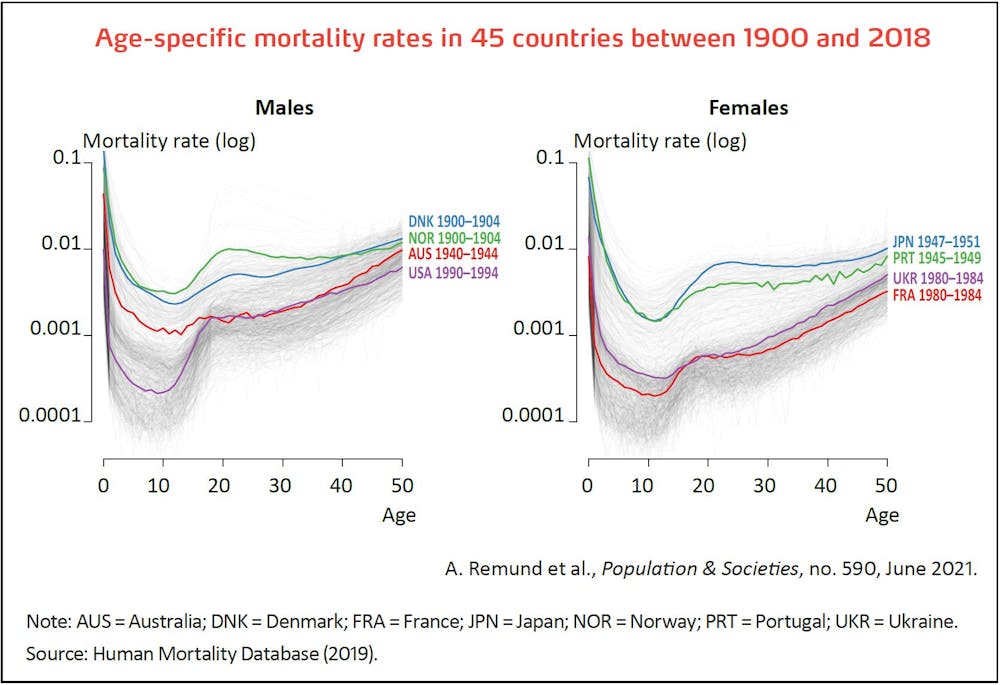
The absolute level of young adult mortality can be surprising. For example, in 1900–1904, the mortality of Danish men was generally similar to or even lower than that of Norwegian men, but with practically none of the excess mortality between ages 15 and 40 observed in Norway. Starting from a much lower level of overall mortality, the curve of American men in 1990–1994 displays pronounced excess mortality, placing them above the absolute level in Australia in 1940–1944, despite a much higher level of overall mortality in the latter country.
Similar observations can be made for women, although they are generally less affected by this excess mortality than men. For example, in the immediate post-war period, while the overall mortality of Japanese and Portuguese women is identical up to age 15, their excess mortality is much higher in Japan above that age. Forty years later, while the absolute mortality rate of French and Ukrainian women was similar between ages 15 and 25, its level reflected high excess mortality in France but not in Ukraine, which has a strong female mortality disadvantage at all other ages. So, it is logical to conclude that for each country pair considered here, young adults are intrinsically more vulnerable in Denmark than in Norway, in the United States than in Australia, in Japan than in Portugal, and in France than in Ukraine, whatever the absolute mortality levels between ages 15 and 30.
Young adult excess mortality seems to be a distinct component of human mortality that stands alongside the other processes governing overall mortality. While called the “excess-mortality hump” because of the bulge it creates in the mortality curve, like that observed for Norwegian males in 1900, it may also resemble a plateau, as observed for American males in 1990 and for French females in 1980. Let us examine the possible causes of this phenomenon.
Historically universal excess mortality?
Young adult excess mortality is considered a worldwide phenomenon particularly prevalent among men. This is because we tend to view adolescence as a naturally tumultuous period, marked by the psychological upheavals associated with puberty*, such as the production of sex hormones or the asynchronous development of different parts of the brain*. It is believed these hallmarks of the “adolescent brain”, as it is sometimes called in the neuropsychological literature, are reflected in a lack of inhibition, excessive risk-taking, impulsiveness, and a general struggle to foresee the consequences of one’s behaviour.
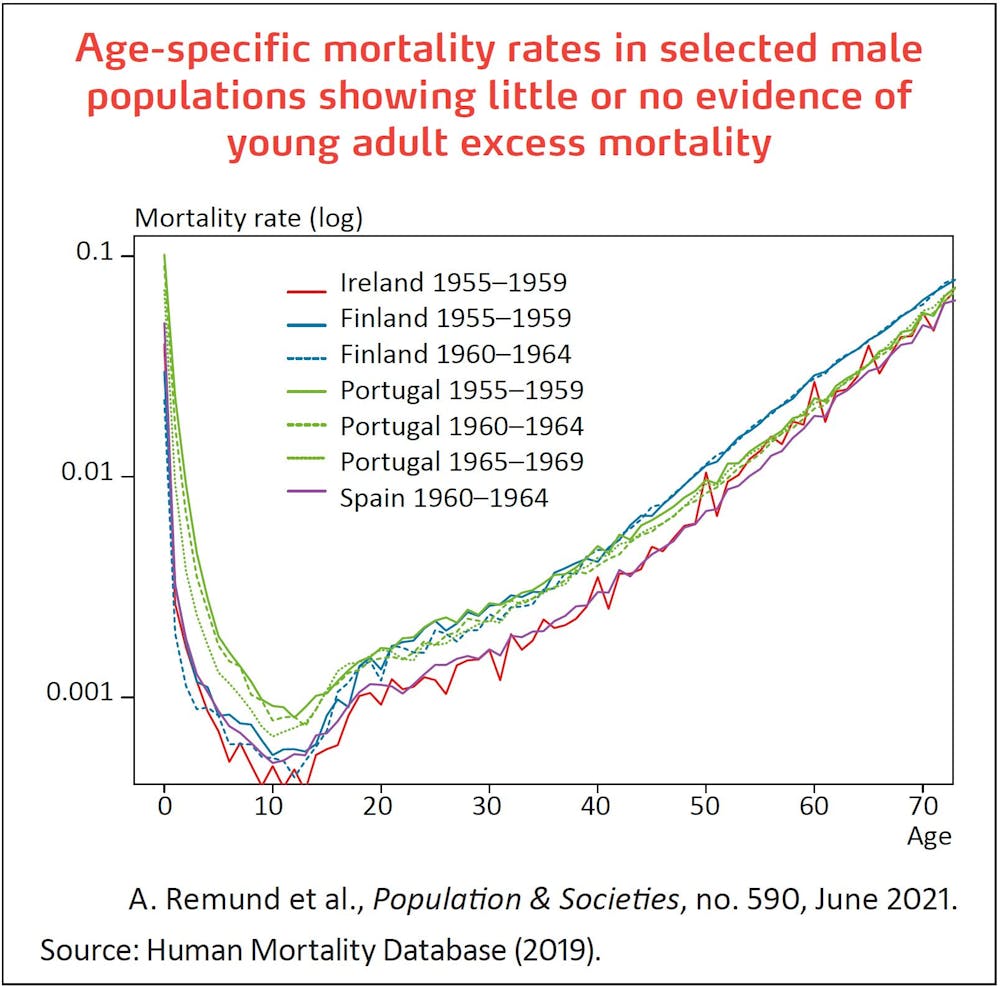
These assumptions are only partially borne out by fact, however. Analysis of several thousand curves similar to those presented in Figure 1 shows that while excess mortality is a frequent reality for men, it is very limited or non-existent in certain cases (Figure 2). Exceptions of this kind were especially common in the 1950s and 1960s, in both Southern Europe (Spain and Portugal) and Northern Europe (Ireland and Finland).
Excess mortality among young women is systematically lower than that of young men, if not non-existent. It is nonetheless widely observed in different contexts, not only in the past, when maternal mortality was still high, but also more recently (Figure 3).
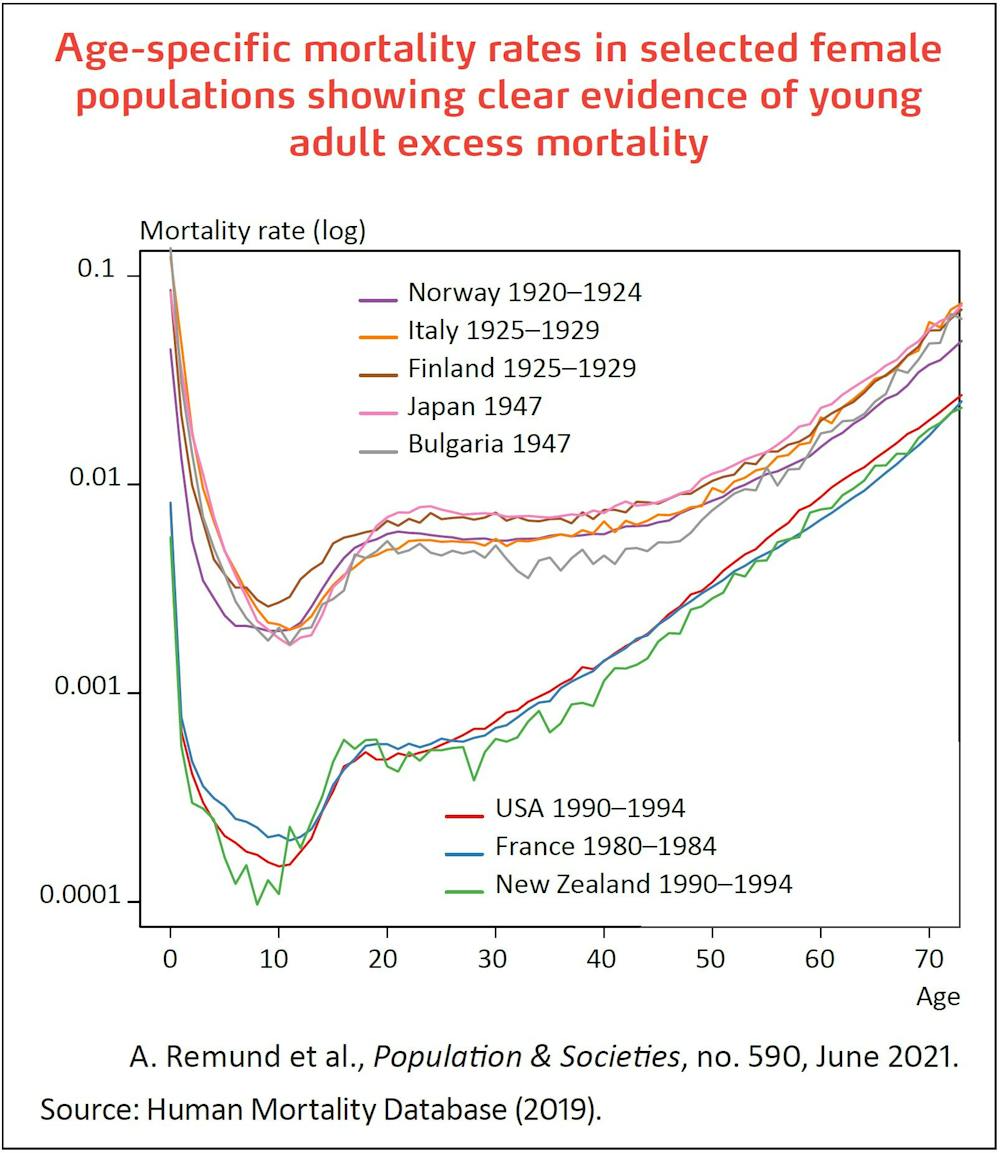
It was especially high in the interwar period, both in Northern Europe (Finland and Norway) and in Southern Europe (Italy), perhaps due to the high incidence of tuberculosis (see below), a common disease after the Second World War in countries such as Japan and Bulgaria. More recently, pronounced excess female mortality among young adults has been observed in several industrialized countries including France, the United States, and New Zealand; only the 1950s and 1960s were free of this phenomenon. The excess mortality hump is thus not universal, and neither is it specific to males.
Live fast, die young?
Another common belief is that youths tend to die in higher numbers because of a greater inclination to take risks in the years after puberty. In the literature, the term “accident hump” is often used, with some authors seeing an explicit link between excess mortality and adolescent risk-taking resulting in more frequent accidental or violent deaths. Here again, this explanation is only partially borne out by fact.
First, regarding the age range concerned, while the hump starts to form in early adolescence, it continues up to age 30 at least – well beyond the end of puberty. In the United States, young adult excess mortality in the 1960s disappeared at around age 35 for men and age 25 for women. This limit then shifted to later ages for both sexes, reaching 45–50 years in the early 1990s, partly because of the HIV epidemic which causes deaths at later ages, on average, than accidents do. Since then, the age limit of the US accident hump has fluctuated between 30 and 40 years, partly because of the current epidemic of opioid overdose deaths. Given the extensive age range covered by the hump, it cannot be attributed to a purely biological factor that leads to high-risk behaviour in adolescence.
Secondly, the breakdown of causes of death linked to the excess mortality hump is more complex than it appears, and while accidents have played an important role in recent decades, they are not always the leading cause of excess mortality at young ages. For example, in the United States, road traffic accidents, which accounted for around 60% of excess mortality in the 1960s, now only explain a quarter of young men’s deaths, on a par with suicides and homicides. For both sexes, the contribution of overdoses to excess mortality has risen from practically 0% to 20% in the last decade.
The role of tuberculosis
Historically, deaths from external causes have not always reached the levels seen in recent years. In the 22 countries, pulmonary tuberculosis was the main cause of excess mortality among youths until the mid-19th century. In the interwar period, the disease still accounted for around 50% of male excess mortality on average, with proportions of up to 90% in Portugal, and ranging from 70% to 90% in Sweden, Spain, France, England, Greece, Italy, the Netherlands, and Norway.
In the same period, maternal mortality accounted for less than 10% of female young adult excess mortality, excepting certain non-European countries (United States, Chile, New Zealand, and Taiwan), where it still represented 30% to 40% before the 1940s. Deaths from external causes (suicides, homicides, accidents including road traffic accidents) overtook tuberculosis deaths between 1940 and 1960, with varying patterns across countries. This turnaround coincides with the development of antibiotics (streptomycin, effective against tuberculosis, was discovered in 1944) and the boom in car ownership. In historical terms, the major role of violent and accidental deaths in young adult excess mortality is a relatively recent phenomenon.
While the young adult excess mortality hump was first spotted 150 years ago, it remains imperfectly understood. It is sometimes the object of misconceptions based on a purely biological conception of adolescence as a universal, gendered phenomenon linked to high-risk behaviour of young adults.
In reality, the hump evolves independently of overall mortality levels, is more pronounced for men than women, and is not universal. It often extends beyond puberty and fluctuates with changes in causes of death not necessarily linked to accidents or violence. While biological factors cannot be excluded, the historical context of the transition to adulthood plays a key role by placing young adults at heightened risk.
This text is adapted from an article by the authors published in Population & Societies, no. 590, “Is young adult excess mortality a natural phenomenon?”